

KZA Telehealth Solutions Center
2024 and Beyond
Up-to-date and comprehensive resources.
*We strongly encourage that you bookmark or save this page for easy access in the future and check back regularly for updates as we learn more.

Last Updated November 16, 2023
2024 CMS Updates to Telehealth

2024 CMS Updates to Telehealth
Last Updated November 16, 2023
Telehealth in 2024 and Beyond

Virtual and On-Demand Education
Now is the perfect time to sharpen up your coding and
reimbursement knowledge with education from KZA.
State Licensure Requirements and Compacts
Federation of State Medical Boards (FSMB): Listing of States Modifying Licensure
Requirements/Renewals for Physicians in Response to COVID-19
Licensure Requirements

Licensure Compacts
What is a license compact?
Please click on the Telehealth Licensure Requirements link for the most updated file.
A license compact is a licensing arrangement where providers can legally practice in other states without having to obtain a separate license for each state participating in the compact. The provider must have an active license in a home state and stay within the licensing scope of practice.
There are several different provider types represented by licensing compacts. See the links above for more information.
Archives
Up to date as of June 14, 2021
FAQs
Added 6/9/2021
Q: How long will the public health emergency (PHE) last?
A: Currently, the PHE is set end on July 20, 2021. However, in a letter to governors earlier this year the Biden Administration indicated that the PHE will likely remain in place through the end of 2021. The letter also indicated that providers would get a 60-day notice before the PHE ends to help prepare for a smooth transition.
Q: Since most states are “getting back to normal”, can we still offer telehealth visits under the public health emergency guidelines?
A: Since the PHE is still in place, ALL flexibilities still apply just as they did in 2020 during the height of the pandemic. You can offer telehealth visits to patients at home, via phone if necessary and on any non-public platform (e.g., Facetime, Zoom, Skype are ok, but Facebook Live and TikTok are not.
Q: Has CMS changed any of the codes lately that can be used during the COVID emergency?
A: CMS has made several changes to the Telehealth Approved List during the course of the public health emergency. The latest additions were made on 4/30/2021. It is always a good idea to check the CMS website frequently for changes. You can find the CMS Telehealth Approved List here.
Q: Have commercial payors stopped covering cost sharing all together?
A: Most commercial carriers stopped covering cost shares in 2020. If fact, we advise that you contact your top 5-6 commercial payors to see what they are and are not covering for telehealth. For example, a payor may have different coverage guidelines for traditional sick visits versus behavioral health, or they may have different end dates or coverage for their different plans.
UPDATED 1/6/2021
Q: What are the documentation rules for telemedicine visits?
A: There aren't any specific rules about documenting telemedicine or telehealth services during the current public health emergency, but the general principles of documentation should be your guide. Remember that medical necessity should be documented, and you should include the following:
Notation that patient consented to the consult held via audio with video or telephone only
Names of all people present during a telemedicine visit and their role
Chief complaint or reason for telehealth visit
Relevant history, background, and/or results
Clinically relevant examination
Assessment
Plan and next steps
Total time spent on medical discussion
UPDATED 1/6/2021
Q: How can we meet a level 4 or 5 new patient visit with the examination?
A: You can document any elements of exam that you inspect or assess through direct observation. Any examination element that requires “hands-on” the patient (palpation, auscultation, etc.) should not be reported. A comprehensive examination requires at least 8 organ systems be documented, and the examination should be performed according to clinical necessity.
That said, for codes 99202-99215 the 2021 E/M Guidelines for new and established patients would now apply. Therefore, the exam would not “count” toward your E/M code level. Although an examination is not required to calculate the level of service a clinically appropriate examination should be documented to support medical necessity and for continuum of care of the patient.
UPDATED 1/6/2021
Q: I am a physical therapist with an NPI. Since I can bill under my name which codes do I use for Online Digital Visits?
A: Physical therapists, occupational therapists, and speech-language pathologists should use the e-Visit codes (98970-98972 for all payors. Although PTs, OTs, and SLPs do have an NPI, they do not bill E/M visits so they should not use (99421-99423). Medicare and most payors are now allowing for PTs, OTs, and SLPs to bill for therapy services under the telehealth waiver for dates of service March 1st through the remainder of the current pandemic. Check with your commercial payors regarding these rules.
PTs, OTs, and SLPs can also bill for telephone codes 98966-98968 as well as virtual check-ins G2250 and G2251 (new for 2021). For E-Visits, telephone assessments, and virtual check-ins, append therapy modifiers GO, GP, or GN as appropriate.
UPDATED 1/6/2021
Q: I heard there is a new diagnosis for COVID-19. If so, what is it?
A: Effective April 1, 2020 use U07.1 for COVID-19.
For all dates of service prior to April 1st, use B97.29 Other corona virus as the cause of diseases classified elsewhere, with any respiratory condition listed as primary.
There are six new diagnosis codes effective January 1, 2021 in light of the ongoing public health emergency. They are as follows:
Encounter for screening for COVID-19 (Z11.52)
Contact with and (suspected) exposure to COVID-19 (Z20.822)
Personal history of COVID-19 (Z86.16)
Multisystem inflammatory syndrome (MIS) (M35.81)
Other specified systemic involvement of connective tissue (M35.89)
Pneumonia due to coronavirus disease 2019 (J12.82)
UPDATED 1/6/2021
Q: What’s the difference between G2012 Virtual Check-In and an (99421-99423) Digital Online Visits? They look the same to me.
A: G2012, G2052, G2250 and G2251 are virtual check-in visits to see if a patient needs to have an E/M service.
Online digital visits (E-visits) are non-video E/M visits that use the patient portal or secure email for the entire visit. Neither of these are telemedicine visits, see definition of a telemedicine visit above.
UPDATED 1/12/2021
Q: Is the HHS pandemic end date still October 23, 2020?
A: No, Secretary Azar of Health and Human Services has extended the current public health emergency (PHE) through April 20, 2021.
UPDATED 10/9/2020
Q: Do we have to use start and stop times or can we use minutes when billing by time?
A: For CMS and some payors exact minutes documented within the permanent record are sufficient, as there is no indication that start and stop times are required for telemedicine visits. You can use start and stop times if you prefer, as long as they are both documented for the visit and are legible.
Some commercial carriers (BCBS and Aetna as of today) want start and stop times documented within the record, according to the latest telehealth guidelines.
ADDED 7/20/2020
Q: Do we add modifier 95 to telephone calls now they are on the CMS approved telehealth list?
A: It depends on the payor and on the MAC. For all Medicare claims the answer is yes, except for First Coast Service Options Inc. First Coast published (in writing) they do not want modifier 95 on telephone claims. For all other payors - review their policies or contact them for further instruction.
ADDED 7/20/2020
Q: Will the upcoming final rule expected in July give us an end date for CMS telehealth coverage?
A: Secretary Azar of Health and Human Services (HHS) determines the end date of the current public health emergency (PHE), not the Final Rule.
ADDED 6/1/2020
Q: If a telehealth visit (real-time audio with video visit) is started and connection is lost or poor, and the rest of the visit is performed by a phone call only – how should we bill this?
A: Medicare clarified this billing scenario on 5/27/2020, saying to bill the code that reflects the bulk of the visit. Meaning that if 5 minutes was spent on a phone call, then 15 minutes spent on the phone to complete the visit, you would bill a 99442 for the 20 minutes, as the bulk of the visit was via the phone.
UPDATED 6/1/2020
Q: What are the new Medicare specimen collection codes for COVID-19, when the test is sent out to a lab?
A: For dates of service March 1, 2020 through the end of the current COVID-19 pandemic, Medicare will cover specimen collection when the test is obtained and sent out to a separate laboratory for processing, when testing is the only service performed on that day. If an E/M service is performed then the specimen collection code is not separately billable as it is considered part of the E/M service.
If specimen collection is the only billable service performed, for Medicare patients you can bill 99211 (for either a new or established patient) for the specimen collection. Some commercial carriers may prefer you use 99000 Specimen collection. Check with your carrier to see which code is billable.
Codes used by laboratories only for collection: G2023 specimen collection for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), any specimen source
G2024 specimen collection for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), from an individual in a SNF or by a laboratory on behalf of a HHA, any specimen source
For a list of the approved codes for COVID-19 testing, see the Coding COVID-19 Testing chart under "Coding Tools & Helps Downloads".
UPDATED 6/1/2020
Q: Our billing company is telling us that Medicare is allowing us to bill E/M codes for telephone only visits. Can we just bill an audio only (telephone visit) with Medicare’s telehealth E/M codes?
A: On April 30, 2020, Medicare added telephone calls (99441-99423) to the approved telehealth services list, however, they are not a replacement for a telehealth E/M (real-time audio and video) visit codes (99201-99215). They clarified that you should bill for 99441-99443 (for physicians, NPs, and PAs) or 98966-98968 (for other qualified healthcare providers) when performing a telephone E/M visit.
Medicare decided to add telephone calls temporarily to the telehealth approved list because some patients don't have access or don't know how to use technology for a virtual face to face visit. They have also increased the wRVU and allowable for 99441-99443 to match the values of 99212-99214 to better reflect the work involved. Telephone calls can be billed for new patients as well as established patients.
So - yes telephone calls can now be billed to Medicare with codes 99441-99443 or 98966-98968 depending on the provider type.
UPDATED 6/1/2020
Q: Are telephone calls the same as telemedicine visits?
A: While telephone calls are now on the telehealth approved list for Medicare, they are not the same as a telemedicine (Medicare calls them telehealth) visits. A telemedicine visit requires both audio and video capabilities in real-time, unlike a telephone call that does not have video capabilities. However, for dates of service March 1st and after, telephone call codes (99441-99443 and 98968-98969) are now a Medicare covered telehealth service temporarily during this public health emergency. Telephone calls are now a reimbursable service when the patient either does not have access to technology or doesn’t have the skill set to use the technology needed for a telehealth visit. Don’t forget to append modifier 95 to the telephone call code since these codes are covered telehealth services during the pandemic.
UPDATED 6/1/2020
Q: What codes can be used for telehealth visits?
A: Any code in the CPT with a gold star (★) can be used as telemedicine/Medicare telehealth visit. Appendix P in the CPT book also has a listing of codes available. This list includes 99201-99215. That said, there are many more codes allowed now during the public health emergency and the CPT book does not list them all. CMS has 251 codes that can be billed as a telehealth visits during the temporary current public health emergency. The CMS published listing is available at https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/Telehealth-Codes.
UPDATED 6/1/2020
Q: Have the guidelines for telemedicine been relaxed regarding "seeing" a patient if the provider is not licensed in the state in which the patient currently resides? (i.e., can a doctor licensed in state A see a patient currently residing in state B?)
A: Yes - the guidelines for seeing patients in another state have been temporarily relaxed during the COVID-19 public health emergency. We suggest contacting your state's regional telehealth center for state-based guidance on this. There has been no end date set as of yet, but be mindful that these changes are temporary. And remember that this temporary flexibility does not apply to any state laws. Be sure and check with any state that you may be seeing patients in before seeing or serving in these areas.
Here is a website that provides a summary of the licensure requirements: https://www.fsmb.org/siteassets/advocacy/pdf/state-emergency-declarations-licensures-requirementscovid-19.pdf
UPDATED 6/1/2020
Q: Do we need a special COVID-19 modifier on our claims to get them paid?
A: It depends – for all telehealth services listed on the CMS Telehealth Services list, you will need to add modifier 95 to the line item on the claim. Other payors may have different modifier requirements, so check with the individual payor.
If the visit qualifies as a no cost-sharing visit, then modifier CS is needed. For dates of service March 18, 2020 through the end of the current public health emergency (date to be determined), Medicare is waiving all cost-sharing for COVID-19 testing and any visits (Medicare telehealth visits and digital online visits only) where COVID-19 testing is ordered or performed. If the visit results in the testing or ordering of a test for COVID-19, use modifier CS to indicate that testing was performed or ordered, and Medicare will pay at 100% of the fee schedule allowable. Cost-sharing is not waived for Virtual Check-In or visits for any other diagnosis or condition. For claims on or after March1st (during the current public health emergency) Medicare advises the use of modifier 95 on all telehealth visits when the visit would have normally been performed face-to-face. This modifier only applies to codes considered telehealth. The complete listing by CMS can be found at https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/Telehealth-Codes.
However, Medicare clarified on 5/27/2020 that modifier CR is not required on any telehealth claim.
Many commercial payors have modifier requirements to indicate the service was provided via telemedicine. See Payor Telehealth Policies for more information.
UPDATED 6/1/2020
Q: We cannot locate a response from any reliable coding resource about how to bill telephone calls lasting more than 30 min. Do you have any guidance on this topic?
A: Telephone calls for both new and established patients have been temporarily added to the approved telehealth list for Medicare for the duration of the COVID-19 public health emergency. Although these codes have been added as telehealth services, they are not billable with the prolonged services codes (99354-99355 for office patients and 99356-99357 for hospital patients). There is no way to bill for additional time with telephone calls. And as a reminder, time calculated should only include the time for the billing provider talking to the patient, not staff time talking to the patient. Commercial payors may have different billing flexibilities during this crisis, so you will want to check with your commercial payors.
Medicare answered this question in their Q &A from 5/27/2020 and affirmed our answer above that there is not a way to bill for phone calls over 30 minutes.
UPDATED 6/1/2020
Q: Can we bill telephone calls to Medicare now that we can’t see the patient face- to- face because of COVID-19?
A: For dates of service March 1st and after, telephone calls (99441-99443 and 98968-98969) are now a Medicare covered service temporarily during this public health emergency. And, the wRVU and reimbursement for telephone calls (99441-99443) has been increased to the values of 99212-99214 respectively.
And as a reminder code G2012 is available for telephone Virtual Check-In calls.
UPDATED 5/1/2020
Q: Can we bill telemedicine visits by time alone?
A: Yes, for Medicare patients the code set 99202-99215, it is appropriate to bill by time. Telemedicine visits can be billed by either MDM or time alone. Medicare updated their policy and will now use the times for each of these codes that are published by the AMA in CPT 2021. Of course, medical necessity is the overarching criterion for all visits and documentation of exact minutes and any clinically appropriate history and examination should be documented in the permanent patient medical record. Contact other payors for guidance on whether or not billing by MDM or time alone is acceptable.
UPDATED 5/1/2020
Q: Can we bill by MDM or Time for hospital services (initial admits and rounds) listed under new Telehealth list of codes?
A: No. Medicare only allows the use of medical decision making (MDM) and time for 99201-99215 office and other outpatient visits when choosing a level of service. But there are several things to remember when choosing a code from the 99202-99215 range:
Time includes the billing provider’s time only on that date including time such as to review imaging studies or outside records (not staff time)
Greater than 50% of time spent in counseling and/or coordination of care is not required for choosing a telehealth visit level (for 99202-99215 only)
CMS time calculations are now the same as the CPT times listed for each code (see below chart)
MDM definition did not change – criteria to meet is still the same
UPDATED 5/1/2020
Q: Can we bill telephone only (99441-99443) calls subsequently during the week (or the same day) for the same patient by the same provider or another provider of the same specialty within the practice if each call is documented properly?
A: Telephone calls have been added to the approved telehealth list for Medicare during the current COVID-19 public health emergency. According to the CPT Assistant, telephone E/M visits:
can only be billed once every 7 days by a single provider or other providers of the same specialty within the same practice (meaning you can bill the telephone call code once per practice per week with providers of same specialty)
can only include time for the billing provider (performing provider(s) if more than one of the same specialty in the same group practice), not staff time on calls
cannot be billed during the post-op global period for a related issue to any procedure/surgery performed
can be billed during the post-op global period for an unrelated issue (not a complication) to the procedure or surgery performed (with modifier 24)
cannot be billed in conjunction with anticoagulant management codes 99363 and 99364 if the call is about warfarin management
cannot be billed "with the domiciliary, rest home, or home care plan oversight services codes (99339-99340) or the care plan oversight services codes (99374-99380) if the call time is used in reporting the care plan oversight service."
For multiple phone calls during the same day with the same patient, you can aggregate the minutes for the calls and bill ONE telephone call code IF ALL of the following criteria are met:
Time calculated is only the time the billing provider is talking to the patient, not nurse or staff time talking to the patient.
Time in exact minutes is documented in the chart for EACH call.
Documentation for each call indicates what was discussed, changed, or added to the plan of care and reason why (if known) for multiple calls (patient is confused, etc.).
Remember - medical necessity for billing any service to Medicare or other payors is based on medical necessity.
For multiple phone calls during a 7 day period with the same patient, you would aggregate the minutes for the calls and bill ONE telephone call code if all the above criteria are met.
UPDATED 4/17/2020
Q: What documentation is needed to bill for a phone only visit besides time?
A: There aren't any specific rules about documenting telephone calls for covered telephone call services during the current public health emergency, but the general principles of documentation should be your guide. Remember that medical necessity should be documented, and you should include the following:
Notation that patient consented to the consult held via telephone
Names of all people present during a telemedicine consultation and their role
Chief complaint or reason for telephone visit
Relevant history, background, and/or results
Assessment
Plan and next steps
Total time spent on medical discussion
UPDATED 4/9/2020
Q: Where can I get comprehensive information about telehealth?
A: KarenZupko and Associates, Inc. (KZA) has a telehealth webinar available on demand and other tools available at http://www.kzanow.com/KZA-telehealth-solution-center. If you require additional assistance, our consultants are here to help. Contact our office at (312) 642-5616 or email info@kzano.com for more information.
UPDATED 4/9/2020
Q: I heard that Medicare patients don’t have to pay their deductible or co-insurance if they have a telemedicine visit. Is this true?
A: For all dates of service March 18, 2020 through the end of the current public health emergency, Medicare is now waiving all cost-sharing for COVID-19 testing and visits where COVID-19 testing is ordered or performed, when a modifier CS is on the claim.
This means that Medicare will pay at 100% of the allowable fee schedule for COVID-19 testing and visits associated with COVID-19 testing. In order to receive payment at 100% coverage for these visits, modifier CS is required on the claim. This change applies to Medicare telehealth visits (commonly performed 99202-99215) and Digital Online visits only. Virtual Check-In is not included and will continue to be paid at the usual rate of 80% of the allowable fee schedule.
For all other covered telehealth visits Medicare is still allowing providers to waive any patient cost-share (e.g., co-insurance, deductible) at their discretion without penalty. This means the provider will only be reimbursed what Medicare pays, if the provider chooses to waive the patient portion of the visit. Many other payors are waiving cost-sharing for telemedicine visits. See Payor Telehealth Policies for more information.
UPDATED 04/9/2020
Q: CMS is saying “E-visit” but not describing a telemedicine visit. Are they the same?
A: CMS is referencing digital online E/M visits (99421-99423) when they refer to “E-visits” in their correspondence. This could change as telehealth evolves, so make sure to look at the codes referenced in the document or alerts you are reading to make sure the definitions or wording they are using has not changed.
UPDATED 4/9/2020
Q: Do you perceive that the spirit of 1135 Waiver which allows providers to waive coinsurance applies to Virtual Check-Ins and/or E-visits as well as Telehealth visits?
A: No. In the Medicare FAQs dated March 17, 2020, they specifically say that the flexibility for providers to waive or reduce cost-sharing to the patient is for telehealth visits only. Virtual Check-Ins and Digital Online Services (E-visits) are not telemedicine and the cost-sharing waiver does not apply to those services. However, on April 7, 2020, Medicare is now waiving all cost-sharing for Online Digital (Evisits) if COVID-19 testing is ordered or performed. They are waiving the cost share for the visit and testing (with the use of modifier CS on applicable line items), but this is only for telehealth visits and digital online services, not for Virtual Check In.
UPDATED 4/9/2020
Q: Have you seen any advisement for providers doing initial evaluations of Nursing Home patients during this crisis? While the established relationship may have been waived, the specific codes are not listed on the List of Telehealth Services. Would G042x be applicable?
A: CMS has updated their list of telehealth services with over 80 new temporarily approved services, and New Patient Nursing Home services (99327-99328) and Established Patient Nursing Home services (99334-99337) are now on the list. Here is the link to the most up to date listing https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/Telehealth-Codes.
UPDATED 4/9/2020
Q: Why would I want to waive the Medicare 20% if the patient has does not have secondary coverage?
A: The benefit is to the patient, not to the practice. Medicare will reimburse 80% of the allowable and 20% of the allowable will transfer to the patient. If the practice waives the 20% because of financial hardship to the patient (meaning the patient can’t afford to pay), the patient benefits but the practice has a negative financial impact.
KZA recommends normal billing processes at this time. If there is a financial hardship and the patient responsibility begins aging, decisions may be made. Take the time now to create a COVID-19 financial payment policy.
NOTE: For all dates of service March 18, 2020 through the duration of the current COVID-19 crisis, Medicare is waiving all cost- sharing for all COVID-19 testing and visits where a COVID-19 test is ordered or performed. Providers must add the modifier CS to the claim, and Medicare will reimburse at 100% of the allowable amount for the telehealth or digital online service (Evisit). This only applies to COVID-19 testing and testing related visits.
ADDED 4/9/2020
Q: Can a Registered Nurse (RN) bill G2012 when communicating with a Medicare patient regarding further evaluation?
A: No, G2012 is not billable by a nurse because a nurse is not a credentialed Medicare provider. Although phone calls are now a covered Medicare benefit, they are only billable by the physician or non-physician provider (PA, NP, CNS) who can bill Medicare for an E/M visit. These services cannot be billed "incident to", since the CPT code requires a physician or non-physician provider.
Check with your commercial payors for payor specific guidance.
UPDATED 4/1/2020
Q: Can a nurse bill a 99211 as “incident to” for a telemedicine visit?
A: If all the “incident to” rules are met and the physician and nurse are in the same suite, yes. Or if all “incident to” rules are met and the nurse and patient are in the same location (office or patient home) and the physician is on a real-time audio with video call then this would also be a billable visit.
UPDATED 4/1/2020
Q: When can we start coding telehealth visits?
A: CMS made the telehealth changes retroactive for Medicare for all dates of service after March 1, 2020. For all other payors, see the Payor Summary chart on our site for published payor specific dates.
UPDATED 4/1/2020
Q: Are G2010-G2012 or 99421-99423 considered telemedicine?
A: No, these codes are not considered telemedicine (no gold star in the CPT). Rather, they are e-visits and virtual check-ins. The distinction is:
Telehealth visits (or telemedicine) allows a clinician (physician, physician assistant, nurse practitioner) to provide a real-time interactive visit via video-chat – that includes both audio and video. Despite CMS adding some therapy codes to the list of covered telehealth services, PTs, OTs, and SLPs are still not eligible to conduct telehealth visits under Medicare.
E-visits are patient-initiated online digital services for new and established patients (e.g. online patient portal). They are represented by CPT codes 99421- 99423 (0.43-1.39 RVUs) for physicians, physician assistants, and nurse practitioners and CPT codes G2061-G2063 (0.34-0.94 RVUs) for other qualified health providers (PTs, OTs, SLPs) and require a modifier GO, GP, or GN on the claim. These services are not considered telemedicine and are not subject to the previous site limitations.
Virtual check-ins allow new and established patients to briefly connect with their clinicians (as defined above) between visits where the communication is not related to a medical visit within the previous 7 days and does not lead to a medical visit within the next 24 hours (or soonest appointment available).
These check-ins can be provided by phone, secure text, portal; 5-10 minutes of medical discussion (G2012 for 0.41 RVUs) or remote evaluation of recorded video and/or images submitted by a patient including interpretation with follow- up with the patient (G2010 for 0.34 RVUs). Both codes can be performed by other qualified health providers (PTs, OTs, SLPs) and require a modifier -GO, -GP, or -GN on the claim.
These services are not considered telemedicine and are not subject to the previous site limitations.
UPDATED 4/1/2020
Q: If PA is seeing a patient in the office, could they still bill a Telemedicine visit under physician as “incident to” if they are not at the same site? Did CMS waive the ‘direct supervision’ guideline during this pandemic?
A: If the performing provider is an NPP (physician assistant, nurse practitioner), we advise billing direct under the NPP’s provider number as billing “incident to” a physician by an NPP has not been formally addressed to date. Remember, the guidelines for “incident to” billing are rather stringent so we typically recommend NPPs regularly bill direct for their services. Billing direct by the NPP will help better utilize their talents as well as provide an opportunity to optimize reimbursement because both the physician and NPP can see patients in tandem.
UPDATED 4/1/2020
Q: If the provider is working remotely from home (temporarily), what would the place of service (POS) be?
A: If billing telemedicine visits (with real-time audio and video) then the POS would be the place of service where the provider would have normally seen the patient (office, or hospital-based clinic, etc.) for Medicare and the address on the claim would be the provider's home address, not the clinic address. Once the provider returns to the clinic he/she can perform telehealth visits and would resume using the clinic address on the claim. That is the CMS requirement for Medicare.
For example, if you would normally have seen the patient in your private practice office then report the E/M code using POS 11. If you would normally have seen the patient in a provider-based clinic in the hospital, then report the E/M code using POS 22.
Don’t forget that Medicare now requires modifier 95 (Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunications System) to be appended to all CPT codes reported for telehealth visits.
Commercial payors may or may not follow Medicare guidelines. See Payor Telehealth Policies for more information.
UPDATED 4/1/2020
Q: We are doing all our telemedicine encounters in our normal exam rooms. The physician and PA are in the same suite. Are we able to bill “Incident-to” then?
A: If the performing provider is an NPP, we advise billing direct under the NPP’s provider number as billing “incident to” a physician by an NPP has not been formally addressed to date. This will help utilize the NPP and provide an opportunity to optimize reimbursement as both the physician and NPP can see patients in tandem.
UPDATED 4/1/2020
Q: We are performing Virtual Check-Ins and Online Digital Visits. Our place of service will be 11. May we bill “Incident-to” now if the provider is in the office?
A: If all “incident to” guidelines are met, then these visits could be billed as “incident to.” Remember new patients, new problems or any changes in the plan of care do not meet “incident-to” guidelines. All visits are patient-initiated and the scheduling staff may not be able to determine if the encounter meets the billing rules. If the performing provider is an NPP, we advise billing direct under the NPP’s provider number as this has not been formally addressed to date.
UPDATED 4/1/2020
Q: What is the place of service for telemedicine visits?
A: For Medicare, on all claims for dates of service March 1, 2020, and forward through the duration of the current public health emergency, use the place of service code where the provider would have normally performed the face-to-face service (e.g., 11, 22, 19, etc.). For example, if you would normally have seen the patient in your private practice office then report the E/M code using POS 11. If you would normally have seen the patient in a provider-based clinic in the hospital, then report the E/M code using POS 22.
If you normally would have performed the service as a telehealth visit, then use place of service code 02. Commercial payors may have different requirements. See Payor Telehealth Policies for more information.
Q: What is the place of service for Virtual Check-Ins and Digital Online Visits?
A: Use your normal clinic place of service (e.g., 11, 22, 19) as these codes are not recognized as telemedicine.
ADDED 3/26/20
Q: Do we have to use modifier “CR” on professional claims during this public health emergency?
A: Not for Medicare claims. CMS clarified this on March 20, 2020, saying modifier CR is not needed under the current blanket waiver. This is a Medicare modifier, but you may want to verify with your commercial payors.
ADDED 3/26/2020
Q: How do we bill for Q3014 when we perform a telemedicine visit with video?
A: Q3014 is not billed by the provider performing the visit (real-time audio and video) when the patient is at a different location. Q3014 is only billed by facilities if a patient goes to a facility and uses the facility’s technology (computer/web service, room) to have a visit with a provider at a distant site (another location – not on the same campus).
ADDED 3/26/2020
Q: Is a physician clinic considered a facility for telehealth?
A: Yes, as long as the patient is at a different physical location than the billing provider. Meaning – the patient can’t be in the same clinic or site as the doctor performing the telemedicine (or telehealth as Medicare calls it) visit.
ADDED 3/26/2020
Q: Is a physician clinic only an originating site under the COVID-19 government waiver?
A: No. A physician clinic has always been an approved originating site (where the patient is located for a telemedicine visit) and that should not change once the waiver has been lifted. However, remember the patient must be at a different physical location than the provider (physician or PA/NP) in order to qualify for a telemedicine/telehealth visit.
ADDED 3/26/2020
Q: I heard there are tools that CMS has for general practitioners. Do you know where to find this?
A: CMS developed two tool kits and can be found through the following links:
Toolkit for general Telemedicine:
https://www.cms.gov/files/document/general-telemedicine-toolkit.pdf
Toolkit for ESRD providers:
https://www.cms.gov/files/document/esrd-provider-telehealth-telemedicine-toolkit.pdf
ADDED 3/26/2020
Q: What’s the difference between “telehealth” and “telemedicine”?
A: Colloquially, the terms tend to be used interchangeably. By definition, telehealth is a collection of technological tools/services, and telemedicine is an audio/video, real-time E/M visit where the provider and patient interact and communicate. CPT has indicated with a gold star (★) codes that can be used with telemedicine. Modifier 95 is defined as “synchronous telemedicine service rendered via a real-time interactive audio and visual telecommunications systems”. However, Medicare refers to “telemedicine services” as the umbrella of services that include “telehealth visits,” “virtual check-ins,” and “e-Visits.”
ADDED 3/26/2020
Q: Do all the new rules for telemedicine visits apply to Medicaid, since it’s a government payor?
A: Medicaid payors fall under individual state authority so they may have different rules or guidance for telemedicine. Check with your state Medicaid carrier for guidance.
ADDED 3/26/2020
Q: Is G2012 for telephone calls or just for the patient portal?
A: Keep in mind that G2012 is not a telemedicine visit but rather a “virtual check-in” service. It is not a telemedicine service because it is not performed with real-time audio and video means. If you are indeed performing a “virtual check-in” visit rather than a telemedicine visit, then G2012 would be appropriate. G2012 can be used for a telephone call (no video) or via the patient portal. This code has been described by CMS as communication to see if a patient needs to make an appointment for further evaluation, not as an E/M service in and of itself.
ADDED 3/26/2020
Q: What does Medicare mean by “soonest available appointment” in the definition of G2010-G2012?
A: CMS did not give a specific definition for this. Use your reasonable judgment for what your practice would normally say is your “soonest available appointment”.
ADDED 3/26/2020
Q: Can smartphones be used for telemedicine visits?
A: Yes as long as you are using real-time audio AND video capability. This is true during the temporary waiver enacted by the government. An end date for this service has not yet been established.
ADDED 3/26/2020
Q: Does telemedicine require special credentialing?
A: No there is no special credentialing required. If you are a provider who can bill E/M services to Medicare under normal circumstances, then you can bill with telemedicine codes.
ADDED 3/26/2020
Q: Now that we aren’t limited to HIPAA compliant software, can we use any app or platform to conduct a telemedicine visit?
A: You may use any app or platform that is not “public-facing” according to HHS. Platforms such as Facebook Live, Twitch, and TikTok are considered public-facing. Skype, FaceTime, Facebook Messenger Chat, and Google Hangouts video are all approved platforms.
ADDED 3/26/2020
Q: Can we bill a telemedicine visit if the patient is in the waiting room behind the glass and the physician is in his office at the time?
A: No. Telemedicine visits are only to be used when the patient is not at the same site as the physician.
ADDED 3/26/2020
Q: Do we have to document in the chart, or keep separate records for telemedicine visits?
A: Documentation rules for services rendered have not changed. All documentation for telehealth services should be documented with appropriate detail in the permanent medical record.
ADDED 3/26/2020
Q: Can we do telemedicine visits through our EHR?
A: Check with your EHR vendor on this. Some offer telehealth services through their system.
ADDED 3/26/2020
Q: Can post-op visits be billed as telemedicine visits?
A: No. Post-op visits are still post-op visits if they are within the global period. If you are seeing the patient for an unrelated (not a complication) problem, then a telemedicine visit can be billed with modifier 24. However, you can see post-op patients via a telemedicine platform and report 99024 as you normally would.
ADDED 3/26/2020
Q: Can Medicare post-op visits be billed as remote check-ins where the patient sends a picture of the incision?
A: No. Guidelines for post-op visits have not changed. Since the check-in is related to the surgery, this is not a billable scenario unless it is outside of the surgical global period.

Updated as of 8/24/2021
Payor Telehealth Policies

We advise you to check with your payors for specific details regarding telehealth coverage, as changes to policies are happening frequently
As of February 2021, we have indications that the current public health emergency will most likely continue through the end of the year, 2021. A final decision has not been put in writing by the acting Secretary of Health and Human Services, so we encourage you to check back frequently for updates.
Last Updated April 30, 2020
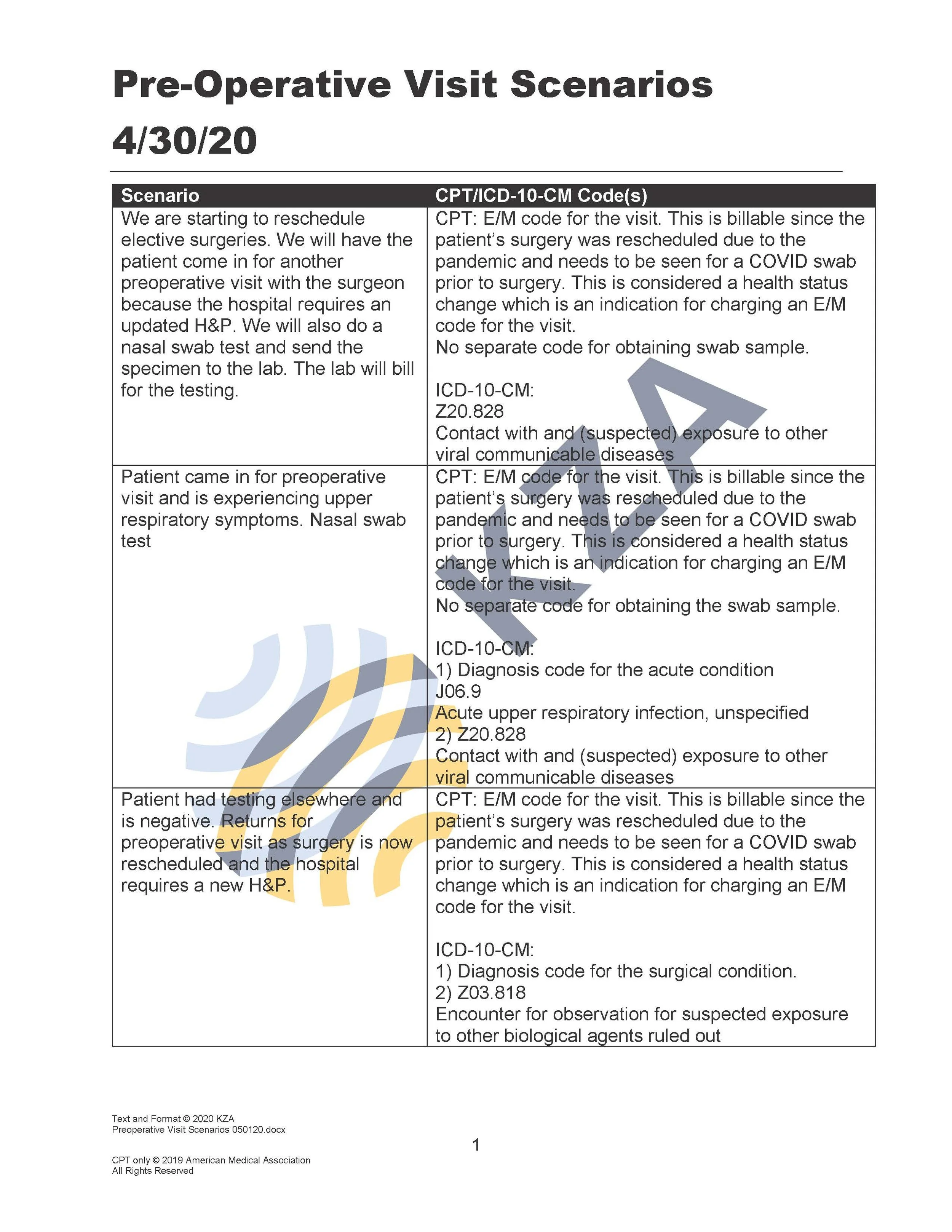
Preoperative Visit Scenarios
Medicare Payment for COVID-19 Diagnostic Tests
Medicare Payment for COVID-19 Diagnostic Tests
Earlier this year, CMS developed two codes that laboratories can use to bill for certain COVID-19 lab tests, including blood tests. CMS has updated its guidance to include payment details for additional CPT codes created by the American Medical Association. There is no cost-sharing for Medicare patients. You can find your local Medicare carrier allowables here:
https://www.cms.gov/files/document/mac-covid-19-test-pricing.pdf

Last Updated October 7, 2020
Telehealth Guide During the Public Health Emergency (PHE)
This article has been updated to reflect continuing changes made by CMS since March 2020. This guide covers the temporary changes made due to the COVID-19 public health emergency (PHE). In order to accommodate the increased demand for patient care while protecting patients and healthcare workers, several key updates have been made. The following information is effective for all dates of service on or after March 1, 2020. At this time there is no permanent end date for these changes, as the PHE is an ongoing event. This could change at any time, so we encourage you to review this information frequently.
Definition of Telehealth and Telemedicine
The terms telehealth and telemedicine tend to be used interchangeably. By definition, telehealth is a collection of technological tools/services, and telemedicine is an audio/video, real-time E/M visit where the provider and patient interact and communicate. CPT has indicated with a gold star (★) codes that can be used with telemedicine. Modifier 95 is defined as “synchronous telemedicine service rendered via a real-time interactive audio and visual telecommunications systems”. However, Medicare refers to “telemedicine services” as the umbrella of services that include “telehealth visits,” “virtual check-ins,” and “e-Visits."
Telemedicine Technology
Effective March 17, 2020, the Office for Civil Rights (OCR) will not impose penalties for noncompliance with the HIPAA Rules in connection with the good faith provision of telehealth during the COVID-19 emergency, regardless of the patient’s diagnosis.
PLEASE NOTE: Separate State action will be required in certain areas – physicians should assess their State-specific privacy laws prior to moving forward.
Where to get started?
Platform selection. CMS allows for use of telecommunications technology that has audio and video capabilities that are used for two-way, real-time interactive communication to conduct Telehealth visits. Which one to use?
Does your EHR vendor offer a Telehealth option? Is it readily available? Realistically how quickly could it be operationalized?
Aesthetic plastic surgery practices: Did you know that Symplast, PatientNow, Modernizing Medicine, Stage4, and Nextech all offer an integrated telehealth platform and/or have preferred vendors? Contact your vendor’s account manager for more details.
During the period of time of the national emergency, CMS is temporarily waiving the enforcement of using HIPAA compliant platforms. Apple FaceTime, Facebook Messenger video chat, Google Hangouts video, or Skype are all options*.
Physicians are encouraged to notify patients that these third-party applications potentially introduce privacy risks, and physicians should enable all available encryption and privacy modes when using such applications.
Another practical consideration – would personal contact information be shared with patients? FaceTime uses a cell phone number, Facebook Messenger video chat uses a Facebook account. A business Skype account could be utilized.
* NOTE: Facebook Live, Twitch, TikTok, and similar video communication applications are public-facing, and should not be used in the provision of Telehealth.
There are HIPAA secure platforms out there like Doxy.me (free version and a paid version with upgraded features), Updox, VSee, Zoom for Healthcare, Google G Suite Hangouts Meet, Rezilient, OrthoLive, Hopdoc, ModMed , PreciseCare, Klara, and OneTouchTeleheath.. Consider posting on or perusing your specialty society’s message boards – we are sure there is a buzz about what everyone else is using.
Equipment Needs. A smartphone will have a built-in camera. Most laptops and many tablets have a built-in camera and microphone. If you will be conducting the visit at a desktop, do you have a webcam and a microphone?
Aesthetic plastic surgery practices: Did you know that Symplast, PatientNow, Modernizing Medicine, Stage4, and Nextech all offer an integrated telehealth platform and/or have preferred vendors? Contact your vendor’s account manager for more details.
Operational Considerations
Telehealth informed consent. Contact your medical malpractice carrier or your specialty society about obtaining a specific Telehealth informed consent (Here’s an example: https://www.thedoctors.com/siteassets/pdfs/risk-management/informed-consent-forms/Telehealth.pdf).
Documentation template for telehealth visits. An example provided to us states: “Patient seen today via Telehealth by agreement and consent of patient in light of current COVID-19 pandemic. I used the following Telehealth technology ___________________________________ (e.g., video, phone call) during the visit. This patient encounter is appropriate and reasonable under the circumstances given the patient’s particular presentation at this time. The patient has been advised of the potential risks and limitations of this mode of treatment (including but not limited to the absence of in-person examination) and has agreed to be treated in a remote fashion in spite of them. Any and all of the patient’s/patient’s family’s questions on this issue have been answered and I have made no promises or guarantees to the patient. The patient has also been advised to contact this office for worsening conditions or problems, and seek emergency medical treatment and/or call 911 if the patient deems either necessary.”
Scheduling. If the office is closed, scheduling telehealth visits would likely follow the same patterns as scheduling in-office visits. However, take a look at how your appointment schedule is ultimately linked to the claim that is generated as the place of service for telehealth may be different (as discussed later).
For those practices who are still seeing patients in the office, managing telehealth visits with in-person visits needs to be considered. It’s likely easier to create a separate appointment type of “Telehealth” to distinguish them from regular visits. Further consider creating different appointment types for “telehealth visit,” “telephone visit,” “e-Visit,” and “virtual check-in.” Also, keep in mind any scheduling reporting/appointment counts you may want to do later. Think of the scheduling set-up from the perspective of all staff – those who will be scheduling the appointments, those who will be “rooming” the patients, the providers, and how it impacts billing.Patient Flow. Determine what patient flow will look like. Where will you physically conduct the Telehealth visit? In an exam room? At your desk? Will you be at home? Who will get the patient “ready” to be seen?
Tech Troubleshooter. Who will be your designated troubleshooter? Inevitably, patients will need some tech help, so proactively assign a tech-savvy staff member to assist.
Payment collection. It’s a delicate time right now. Medicare is allowing, but not requiring, coinsurance and deductible amounts to be waived. Some payors have eliminated cost-sharing requirements for telehealth visits. See the Payor Summary chart for details. For patients who have patient responsibility amounts, perhaps a prudent choice is to allow for online payments and/or sending the patients a bill for the services after the telehealth visit.
Billing Considerations
What kind of visit is it?
There are many types of services that can be performed remotely during the public health emergency (PHE). For a complete listing of approved telehealth service for Medicare click here. Below are the most common types of modality used (audio+visual, phone, patient portal) is the driving determination of what kind of visit it is.

Telemedicine visits (and telephone visits temporarily) typically have the highest reimbursement, followed by e-visits, and virtual check-ins. When determining which services to provide virtually, consider cost, resources, technology, continuity of care, and reimbursement for those services.
Place of Service (POS)
There are two major new points:
Effective March 1, 2020, during the COVID-19 public health emergency, use the place of service where the provider would normally have performed the visit if the patient had been seen face-to-face (e.g. 11 or 22), NOT POS 02 for all CMS telehealth and telephone services. For example, if you would normally have seen the patient in your private practice office then report the Evaluation and Management (E/M) code using POS 11. If you would normally have seen the patient in a provider-based clinic in the hospital, then report the E/M code using POS 22. If you normally would have performed the service via telehealth means, then use POS 02 on the claim.
And append modifier 95 (Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunications System) for all telemedicine visits on Medicare claims (no modifier 95 on e-Visits, virtual check-ins, and telephone calls as these services are not telemedicine.) This allows Medicare to pay these visits at the higher Non-Facility fee schedule rate when applicable. CMS does allow providers to continue to use POS 02 for all telehealth services, however, this will result in decreased reimbursement under the Facility Fee Schedule. Commercial payors may have different guidelines. For all other payors, see the Payor Summary chart on our site for published payor guidelines.
TIP: File corrected claims for telehealth services that have already been billed to update the place of service. You might want to hold on to your non-Medicare claims for a few days to see if these payors will now follow Medicare’s new guidelines.
If the provider is furnishing the telehealth service from their own home, list the provider’s home address in Box 32 service location on the claim. The place of service is still the same place of service the provider would normally see the patient (office, or hospital-based clinic, etc.) and the address on the claim would be the provider’s home address, not the clinic address.
Choosing an Outpatient/Office E/M Code (99201-99215) – MDM or Time
Medicare now says that the appropriate E/M code for the telehealth visit (real-time audio and video) may be chosen based on Medical Decision Making (existing guidelines – not the new 2021 guidelines) or total amount of time. This is good news for surgeons who oftentimes must choose a lower level E/M code because the Examination component is not met. Be sure to have good documentation of the MDM or time – whichever you use to choose the level of billed E/M code.
Modifiers
95: Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunications System: Note: Medicare now temporarily requires modifier 95 on all claims for telehealth visits that would normally be performed as face-to-face visits such as an office visit.
GQ: Via asynchronous telecommunications system. Clinicians participating in the federal telemedicine demonstration programs in Alaska or Hawaii must submit the appropriate CPT or HCPCS code for the professional service along with the modifier GQ “via asynchronous telecommunications system.”
For other telehealth modifiers see the KZA Modifier matrix under “Coding Helps and Tools Downloads”.
Note: Medicare stopped the use of modifier GT (Via interactive audio and video telecommunication systems) in 2017 when the place of service code 02 (Telehealth) was introduced. However, many private payors are still using the modifier GT. See the Payor Summary chart for reference.
Physician Supervision
CMS has temporarily augmented the definition of direct physician supervision to include virtual supervision. During the current public health emergency, the provision requires that the physician use real-time audio with video technology while supervising.
Originating Site
During the COVID-19 public health emergency, rural and site limitations are removed. Home is temporarily an approved site (during the COVID-19 pandemic). Telehealth services can now be provided regardless of where the enrollee is located geographically and regardless of the type of facility.
Physicians do not report Q3014 (Telehealth originating site facility fee). This code is used by an originating site separate from where the physician is located when performing traditional telehealth services pre-public health emergency rules. Refer to the above discussion on place of service (POS) codes.
Note: Locations that are newly eligible will not receive a facility fee.
Telephone Only Services – Medicare Now Pays 99441-99443 and 98966-98968
Telephone only E/M visits are now approved for new and established patients. These codes were previously non-covered and not payable by Medicare. But at this time due to the COVID-19 pandemic, Medicare will reimburse for these services. Additionally, while CPT states these codes are for established patients, Medicare is allowing telephone only E/M codes for new patients.
Physicians and NPPs (e.g., physician assistant, nurse practitioner) that bill under their own NPI should use 99441-99443 while “qualified non-physician health care professionals” such as physical and occupational therapists, speech-language pathologists, registered dieticians, and social workers should use codes 98966—98968. CMS also requires that therapists use the appropriate therapy modifier (GO, GP, GN) for their services
ALERT: Do not bill 99201-99215 for telephone only E/M, as these codes still require real-time audio and video. Some private payors allow the billing of 99201-99215 for telephone only service. Check your individual payor policies for guidance.
Virtual Check-In
G2010 Remote evaluation of recorded video and/or images submitted by an established patient (e.g. store and forward), including interpretation with follow-up with the patient within 24 business hours, not originating from a related E&M service provided within the previous 7 days nor leading to an E&M service or procedure within the next 24 hours or soonest available appointment
G2012 Brief communication technology-based service, e.g. virtual check-in, by a physician or other qualified health care professional who can report E&M services, provided to an established patient, not originating from a related E&M service provided within the previous 7 days nor leading to an E&M service or procedure within the next 24 hours or soonest available appointment; 5-10 minutes of medical discussion
Consider the following guidelines when billing the below codes:
Can now be billed by PTs, OTs, SLPs, LCSWs, and clinical psychologists, if needed. CMS also requires that therapists use one of the following modifiers for these services: GO, GP, or GN
Can be any real-time audio (telephone), or "2-way audio interactions that are enhanced with video or other kinds of data transmission"
During current public health emergency (PHE) can be a new or established patient
Any chronic patient who needs to be assessed as to whether an office visit is needed
Patients being treated for opioid and other substance-use disorders
If an E/M service is provided within the defined time frames, then the telehealth visit is bundled within that E/M service
No geographic restrictions for patient location
Should be initiated by the patient since a co-pay is required. Verbal consent to bill and documentation is required
Communication can use non-HIPAA compliant technology during the COVID-19 public health emergency
Not considered a telemedicine service so does not need modifier 95 for Medicare claims
Online Digital Evaluation & Management (E/M) or e-Visits
99421 Patient-initiated digital evaluation and management service, for an established patient, for up to 7 days, cumulative time during the 7 days; 5-10 minutes
99422 11-20 minutes
99423 21 or more minutes
NOT used for: Non-evaluative electronic communication of test results, scheduling of appointments, or other communication that does not include E/M.
Other notes for using 99421-99423 codes:
Must be through HIPAA-compliant secure platforms, such as electronic health record (EHR) portals, secure email, or other digital applications
During current public health emergency (PHE) can be a new or established patient
Performed asynchronously and audio/video phone can be used (not a traditional telephone)
Must be patient-initiated
The patient must be informed and, the information documented in the chart
Cost-sharing applies to the E/M service; deductible still applies
Use only once per 7-day period
Clinical staff time is not calculated as part of cumulative time
Service time must be more than 5 minutes
Do not count time otherwise reported with other services
Do not report on a day when the physician or other qualified health care professional reports E/M services
Do not report when billing remote physiologic monitoring (RPM), Chronic Care Management (CCM), Transitional Care Management (TCM), care plan oversight (CPO), and codes for supervision of patient in home, domiciliary or rest home, etc. for the same communication
Do not report for home and outpatient international normalized ratio (INR) monitoring when reporting 93792, 93793
Not considered a telemedicine service so does not need modifier 95 for Medicare claims
For healthcare professionals that don’t bill directly to Medicare for E/M services:
Use these codes for Medicare patients only when an online assessment, such as using the patient portal, is being performed by a non-physician profession such as PTs, OTs, SLPs, LCSWs, and clinical psychologists, if needed. CMS also requires that therapists use one of the following modifiers for these services: GO, GP, or GN
G2061 Qualified non-physician professional online assessment (such as using the patient portal), for up to 7 days, 5-10 minutes cumulative time during the 7 days
G2062 11-20 minutes
G2063 21 or more minutes
Remote Monitoring - No change for COVID-19
99453 Remote monitoring of physiologic parameter(s) (e.g., weight, blood pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of equipment
99454 Remote monitoring of physiologic parameter(s) (e.g., weight, BP, pulse oximetry, respiratory flow rate) initial; device(s) supply with daily recording(s) or programmed alert(s) transmission, each 30 days
99457 Remote physiologic monitoring treatment management services, 20 minutes or more of clinical staff, physician, or other qualified health professional time in a calendar month requiring interactive communication with the patient/caregiver during the month
Established or new patients
For both chronic and acute conditions
Can now be provided if patient has only 1 disease process
If monitoring is for treatment of COVID-19 or suspected COVID-19, Medicare allows the service to be reported if more than 2 days and less than 16 days (all other conditions require monitoring of 30 days)
Patient initiated
Involves "asynchronous transmission of healthcare information" from the patient
If an E/M service is provided within the defined time frames, then the telehealth visit is bundled in that E/M service
Follow-up can be by phone, audio/video, secure text messaging, email or patient portal communication
Should be initiated by the patient since a copay is required. Verbal consent to bill and documentation is required
Communication must be HIPAA compliant
This is distinct from CCM code 99490, which can be provided without the patient's presence and use any means of communication
Not considered a telemedicine service so does not need modifier 95 for Medicare claim
COVID-19 ICD-10-CM Guidance
If you are diagnosing and/or treating a patient with COVID-19 is important to use the appropriate ICD10CM codes. Effective April 1, 2020 use U07.1 for COVID-19 once the patient is diagnosed. Prior to April 1st dates of service use B97.29 Other corona virus as the cause of diseases classified elsewhere, listed secondary with any respiratory condition (examples below) listed as the primary diagnosis.
J12.89 Other viral pneumonia
J20.8 Acute bronchitis due to other specified organisms
J80 Acute respiratory distress syndrome
J98.8 Other specified respiratory disorders
If the patient has known exposure, use the applicable exposure codes:
Z03.818 Encounter for observation suspected exposure to other biological agents ruled out
Z20.828 Contact with and suspected exposure to other viral communicable diseases
For signs and symptoms outside of any exposure, use appropriate codes:
R05 Cough
R06.02 Shortness of breath
R50.9 Fever, unspecified
NOTE: Do NOT use B34.2 (coronavirus infection, unspecified) because COVID-19 would not be unspecified.
COVID Telehealth Timeline
Updated April 15, 2022

2022 CMS Makes Major Changes to Telehealth
Updated April 15, 2022
Some telehealth waivers in place for an additional 151 days after the end of the public health emergency.
President Biden signed the Consolidated Appropriations Act of 2022, into law on March 15, 2022. Included in the law is an extension to some telehealth flexibilities for an additional 151 days after the end of the current public health emergency (PHE).
Flexibilities that will be extended include:
Originating site and geographic location waiver – this allows patients to have a telehealth visit from their home (or another site) not just CMS designated originating sites
Extends temporary qualifying providers (e.g., physical therapists, occupational therapists, speech language pathologists, audiologists, and dieticians) the option to furnish distant site services
Mandates CMS to continue covering audio-only telehealth visits for Medicare beneficiaries
Delays the in-person visit requirement for mental telehealth visits for an additional 151 days
POS 10 Telehealth Provided in Patient’s Home
Patient is located in their home (which is a location other than a hospital or other facility where the patient receives care in a private residence) when receiving health services or health related services through telecommunication technology.
Home may be defined to include temporary lodging (hotels, homeless shelters) and patient travels of short distance from the exact home location.
Effective January 1, 2022.
Implementation date of April 4, 2022 for Medicare will not deny POS 10, but will treat it as POS 02. Added for insurance industry use – Medicare does not see a need for POS 10 at this time (as of 4/6/2022). Check with your local MAC and commercial carriers for specific guidance.
POS 02 Telehealth Provided Other than in Patient’s Home
Patient is not located in their home when receiving health services or health related services through telecommunication technology.
A location such as a hospital or other facility
During the PHE, POS 02 is used for providers who do not normally see patients in an office setting.
For use by all providers after the PHE or as directed by the payor during the PHE.
Modifier 93 Synchronous telemedicine service rendered via telephone or other real-time interactive audio-only telecommunications system
Used for real-time, audio-only medically necessary E/M visits.
Communication during the telemedicine service must meet the key components and/or requirements of the same service when rendered via a face-to-face interaction.
Medicare has not given guidance on use of this modifier (as of January 19, 2022).
Check with commercial payors for guidance on usage of this modifier.
Other Medicare modifiers (specifically for telehealth mental health)
FQ – A telehealth service was furnished using real-time audio-only communication technology
FR – A supervising practitioner was present through a real-time two-way, audio/video communication technology
Medicare will give instructions on the use of these modifiers at a future date.
Good News
Medical nutrition therapy (MNT) and diabetes self-management training (DSMT) may be provided via telehealth by registered dieticians and nutrition professionals as distant site providers.
Behavioral health wins: no geographical restrictions, patient’s home can be an originating site, and telephone calls are payable under certain conditions.
The Not So Good News
Not allowing virtual supervision after the PHE ends. CMS will possibly revisit virtual supervision at another time.
CMS declined to add telephone only codes 99441-99443 to the permanent list (except for behavioral health).
CMS Approved Telehealth Listing Updates
CMS created different categories for the Telehealth approved listing to represent three different types of approval categories. For 2022 they have added codes and extended Category 3 codes until December 21, 2023. A word of caution here – if the PHE ends before December 31, 2023, category 3 codes must still meet geographic restrictions and the patient’s home will no longer be an eligible originating site (except for behavioral health).
Category 1 – 109 codes that are permanently approved to stay on the list after the end of the PHE
Category 2 – 99 codes that are temporarily approved until the end date of the current PHE
Category 3 – 64 codes that are temporarily approved until December 31, 2023
A complete updated listing of the approved codes for telehealth can be found at:
https://www.cms.gov/Medicare/Medicare-General-Information/Telehealth/Telehealth-Codes
Telephone Only Telehealth Visits
CMS confirmed that audio-only (telephone call) visit coverage for telehealth visits (99441-99443) will end at the end of the PHE. There are other non-telehealth designated audio-only services, but telephone calls will no longer be considered for payment as telehealth visits.
Originating Site Restrictions
CMS also confirmed that except for behavioral health services, geographic flexibilities will stop at the end of the PHE. This means the patient’s home will no longer be a billable location for telehealth. There are a few exceptions. The patient’s home can be an originating site for behavioral health services, qualifying patients receiving home dialysis with ESRD, and certain patients who are receiving opioid or substance abuse treatment.
Virtual Direct Supervision
In 2021 CMS clarified the definition of virtual direct supervision as audio with video, not audio only communication with a patient. And they confirmed that virtual direct supervision is approved through the end of the year that PHE has ended. In 2022 CMS finalized that virtual supervision will stop at the end of the PHE, but it may be considered again in the future at some point in time.
Virtual Check-In
In 2022 CMS permanently adopted the virtual check-in code G2252 for providers who bill E/M services (e.g., MD, DO, PA, NP)
o G2252 Brief communication technology-based service, e.g., virtual check-in, by a physician or other qualified health care professional who can report evaluation and management services, provided to an established patient, not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 11-20 minutes of medical discussion
All other Virtual Check-In codes remain available for use in 2022.
Online Digital Assessment
As a reminder, the G2061-G2063 code set was deleted in 2021 by CMS. All providers who do not bill E/M services are now instructed to use codes 98970-98972 for online digital assessments.
Originating Site Reimbursement
Q3014 Originating site reimbursement increased in payment for 2022 to $27.59 (from $27.02). Remember, this is the code for hosting the session where the patient is located. This code is not billed by the provider at a distant site who is billing separately for the telehealth visit.

• General principles of documentation still apply
• It’s a shift, not a new standard
• Reason for service is still necessary
• Don’t overgeneralize the note
• Remember to document the rationale in your thinking
• Beware of note bloat
• Don’t copy & paste – still a no-no
• More documentation doesn’t always mean a higher code
• Be intentional with documenting key information
• Key elements for telehealth service documentation:
o Consent
o Patient and provider location
o Names of who is participating in the call
o Audio with video or audio only
o Date the patient was last seen
o Time or Medical Decision Making
Currently there are several bills in Congress regarding telehealth that have passed through the Senate or House of Representatives awaiting next steps.
Telehealth has been brought to the forefront and utilized out of necessity. This has created a lot of attention and scrutiny at both the federal and state levels. There is a vested interest in promoting telehealth and creating healthy broadband infrastructures to increase access for all Americans, especially those in underserved areas throughout the country.
As a result, CMS is forming a “commissioned study” to analyze claims data to
Look at the impact of temporary expansion of telehealth codes
To have feedback for future rulemaking
To mitigate and prevent fraud, waste, and abuse
Telehealth Resources
KZA Telehealth Solutions Center
https://www.karenzupko.com/KZA-telehealth-solution-centerCenter for Connected Health Policy
https://www.cchpca.orgNational Consortium of Telehealth Resources Center
https://www.telehealthresourcecenter.org/
COVID -19 Related Modifiers
Updated February 2, 2023

Published Articles
6 Easy Ways Physicians Can Enhance Your Telemedicine & Video Conferencing Presence
By Jennifer O'Brien
May 20, 2020

Embracing Telemedicine into Your Otolaryngology Practice Amid the COVID-19 Crisis: An Invited Commentary
Kim Pollock, Michael Setzen, and Peter F. Svider
Am J Otolaryngol. 2020 Apr 15 : 102490.
doi: 10.1016/j.amjoto.2020.102490 [Epub ahead of print]
PMCID: PMC7159874
PMID: 32307192
Journal of Orthopaedic Experience and Innovation
Telehealth Visits during the COVID-19 Pandemic
This article focuses on how to maneuver through billing and documentation of telehealth services during the current COVID-19 pandemic. The information discussed is based on the temporary guidelines and changes made by CMS1 and HHS2.

Telehealth vs. In-Person Documentation - the Same, only Different
Jennifer Bell
This article provides clarification according to documentation best practices as of July 29, 2020 under the temporary coding and billing flexibilities for outpatient telehealth visits. Few changes are expected until October, when HHS Secretary Azar revisits the need to renew or end the current public health emergency.

Challenges to Recognizing Revenue for Telehealth Visits
Revenue recognition is difficult at the best of times, if the number of resources on the topic across the Internet are any indication. BDO has put together a guide to make it easier.

Telemedicine During and Post-COVID 19: The Insights of Neurosurgery Patients and Physicians
COVID-19 has caused a massive surge in telemedicine utilization as patients and physicians tried to minimize in-person contact to avoid the spread and impact of the pandemic.
ATA COVID-19 Response Webinar Series
Complimentary ATA COVID-19 Response Webinar Series: Lessons Learned on Billing in the Age of COVID
“The genie is undoubtedly out of the bottle” according to the results of KZA’s Telehealth Payment Pulse Survey.
Neurosurgeons, Orthopaedic Surgeons, Otolaryngologists, and General Surgeons are the majority of the nearly 300 respondents. Interesting takeaways and intel for you to use.
Survey Overview and Key Trends
Myth Busters: Four Common Misbeliefs
Seven Telehealth Coding Tips
Payment Snafus and Denials
Closing Insights
Karen Zupko and Jennifer Bell are lively presenters, eager to share the survey results and how they may impact your practice or organization.

What You Need To Know about Telehealth Documentation and Coding
Jennifer Bell is a CPC credentialed consultant who also is Certified by the Healthcare Compliance Association. As a consultant and auditor with KZA, she has audited over 60 telehealth notes and knows firsthand how to improve documentation—she’s coached nearly a dozen physicians and their staff on needed changes. During this webinar, she discussed the latest information ensuring that your claims process quickly and result in payment.
Topics covered include:
Essential Code Sets: Who can do what and where
Coding With Modifiers
The Dos and Don’ts of Documentation
Busting Myths About Telehealth Coverage for hospital services and phone calls
Commercial Carrier Update
Look into the Crystal Ball for the post-pandemic telehealth future
CCHP Telehealth
Policies
CCHP is all about making telehealth policy more accessible to everyone. We track and compile telehealth-related laws and regulations across all 50 states and the District of Columbia, as well as at the federal level. Our free Policy Finder database is updated consistently throughout the year. Please note: this information should not be construed as legal counsel. Consult with an attorney if you are seeking a legal opinion.

Telehealth During vs. Post Pandemic
Last Updated August 11, 2023

ATA FS Comparison Telehealth Codes
Reviewed November 15, 2023
