

KZA Articles
Explore our featured articles to gain deeper understanding and insights into your specific field of interest or expertise.
Looking for something specific? Utilize our search feature by typing in a key word!
Why a Medical Record Audit is Essential to Your Organization
Coding audits are often viewed as something practices turn to only after a problem surfaces—a payer denial spike, an unexpected audit letter, or a compliance concern. But this reactive mindset carries significant risk. In today’s regulatory and reimbursement environment, waiting for an issue to appear before taking action is no longer a safe strategy.
Deborah Grider, CPC, CPC-I, CPC-P, COC, CPMA, CEMC, CCS-P, CDIP, Executive Consultant
Karen Zupko and Associates, Inc.
Audits Are No Longer Just an Option
Coding audits are often viewed as something practices turn to only after a problem surfaces—a payer denial spike, an unexpected audit letter, or a compliance concern. But this reactive mindset carries significant risk. In today’s regulatory and reimbursement environment, waiting for an issue to appear before taking action is no longer a safe strategy.
Coding audits help practices identify compliance vulnerabilities before payers, auditors, or regulators do. They also reveal something many organizations overlook: not just risk, but lost revenue. Errors in coding and documentation don’t only create exposure—they can quietly undermine financial performance as well.
The Compliance Case for Auditing
Healthcare organizations that bill Medicare, Medicaid, and commercial payers operate in a highly regulated environment, where expectations for accuracy and documentation are clearly defined and actively enforced. Compliance is not optional—it is an operational requirement.
The Office of Inspector General (OIG) has long emphasized that an effective compliance program must be active, not theoretical. It is not enough to document policies in a binder or on a shared drive. Organizations are expected to monitor, evaluate, and continuously improve their processes.
Auditing and monitoring are central components of this expectation. They allow organizations to identify risks early, assess whether coding and documentation practices align with current requirements, and demonstrate a good-faith effort toward compliance.
Waiting until an external entity identifies a problem can have serious consequences. Repayment demands, financial penalties, corrective action plans, and operational disruption can follow—often at a much higher cost than proactive internal review.
As outlined in the OIG’s General Compliance Program Guidance, healthcare organizations are encouraged to implement a structured compliance infrastructure that includes regular auditing and oversight activities. These efforts signal not only diligence but accountability.
Compliance Is Active, Not Passive
Compliance is not achieved by avoiding problems—it is achieved by actively seeking them out and correcting them before they escalate.
Why “We Haven’t Had a Problem Yet” Is Not a Strategy
The absence of known issues does not indicate the absence of risk. It often reflects the absence of visibility.
Auditing Before Someone Else Does
Internal audits put the organization in control of its own narrative, allowing it to address issues proactively rather than reactively.
What Can Happen If You Don’t Audit?
The issue isn’t whether mistakes happen. In busy practices, they do. The real question is whether your organization has a process in place to find, correct, and prevent those mistakes over time.
Without regular auditing, coding errors can compound. Small inconsistencies in documentation, code selection, or modifier usage may seem insignificant at first, but over time, they can create measurable compliance exposure or financial impact.
Overcoding can trigger repayment obligations and increase audit risk. Undercoding, on the other hand, leaves earned revenue uncollected—quietly affecting financial performance quarter after quarter.
Under documentation presents another challenge. Even when care is appropriately delivered, insufficient documentation can make those services difficult to defend in the event of a review.
Modifier misuse can also draw payer scrutiny, particularly when patterns suggest confusion or inconsistency in application.
Perhaps most importantly, problems identified by external auditors are almost always more stressful, disruptive, and expensive to resolve than issues discovered internally. External findings often come with deadlines, financial implications, and reputational concerns that could have been mitigated with earlier intervention.
Auditing provides that intervention. It turns uncertainty into insight and gives practices the tools to respond before issues grow.
Audits Are Not Just About Risk. They’re Also About Revenue.
One of the most common misconceptions about coding audits is that they exist solely to detect overcoding. While identifying compliance risk is an important goal, it is only part of the picture.
In reality, audits frequently uncover undercoding, missed services, incomplete documentation, and underutilized modifiers—all of which can negatively affect revenue. These gaps are often less visible but equally important.
Lost Revenue Can Hide in Plain Sight
Every missed code, incomplete note, or overlooked modifier represents work that was performed but not fully captured. Over time, these small losses can accumulate into meaningful revenue gaps.
Undercoding Is a Compliance and Revenue Problem
Undercoding is often viewed as a conservative or “safe” practice, but it also carries risks. It misrepresents the complexity of care delivered and can affect both reimbursement and data accuracy.
Accuracy Protects Both Sides of the Equation
A strong audit program connects coding accuracy with revenue integrity. Proper documentation and appropriate code selection ensure that services are supported, defensible, and reimbursed correctly.
The goal is not to code higher. The goal is to code correctly, document clearly, and capture the work that was actually performed. By reframing audits as both a compliance safeguard and a revenue integrity tool, organizations can shift from a reactive posture to a proactive strategy—one that supports financial performance, regulatory confidence, and operational strength.
After 40 years of helping healthcare practices improve coding accuracy, documentation quality, and compliance programs, KZA has seen firsthand how proactive auditing strengthens the entire organization. A well-executed audit does more than review charts—it provides clarity, direction, and confidence.
Importantly, a good audit should never feel punitive. The most effective audits are educational, actionable, and tailored to the practice's unique workflows, specialties, and challenges. For four decades, KZA has helped organizations understand not just what went wrong, but why it happened—and how to fix it in a sustainable way.
Contact Us for Expert Coding Guidance
SAVE 5%
Take advantage of our anniversary, save 5% off your audit if contract is executed before June 30th!
312.642.5616
Don't Leave Money on the Table: Medical Necessity Matters
Medical necessity is a foundational principle in healthcare delivery and reimbursement, “Medical necessity is a legal doctrine, related to activities which may be justified as reasonable, necessary, and/or appropriate, based on evidence-based clinical standards of care.”
Deborah Grider, CPC, CPC-I, CPC-P, COC, CPMA, CEMC, CCS-P, CDIP, Executive Consultant
Karen Zupko and Associates, Inc.
Medical necessity is a foundational principle in healthcare delivery and reimbursement, “Medical necessity is a legal doctrine, related to activities which may be justified as reasonable, necessary, and/or appropriate, based on evidence-based clinical standards of care.”
Medical necessity and payment are determined by what the payor will reimburse. For example, many payors, including Medicare and Medicaid, have coverage policies that determine which procedure and diagnosis codes are covered for diagnostic or surgical procedures. If the diagnosis code is not listed in the policy, the payor may determine that the procedure is not medically necessary for that condition.
According to section 1862(a) (1)(A) of the Social Security Act, Medicare will not cover services that “are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member.”
For Evaluation and Management Services
CMS states: “Medical necessity of a service is the overarching criterion for payment in addition to the individual requirements of a CPT code. It would not be medically necessary or appropriate to bill for a higher level of evaluation and management service when a lower level is warranted. The volume of documentation should not be the primary factor in determining the specific level of service billed. Documentation should support the level of service reported."
When billing E/M (Evaluation and Management) services, the practitioner should pause and critically evaluate; based on the presenting problem(s), conditions managed, and/or comorbidities, what level should they bill? The diagnosis codes reported on the claim, the complexity of these conditions, and the management of the condition play a part in the level of service billed. Of course, the selected level of service should be appropriately documented.
Many payors are now using automated technology in downcoding of E/M services from levels 4 and 5 to level 3 based on the diagnosis code, often using AI to make this determination. The payor does not see the documentation. Accurate diagnosis coding is critical to support medical necessity for these higher levels of service.
Diagnosis Coding Is Important in Demonstrating Medical Necessity
Surgeons or specialists who treat a patient many times don’t code the comorbidities that affect patient management, such as diabetes, COPD, Hypertension, etc. This is a significant oversight. If a condition influences clinical decision making, risk assessment, or treatment planning, it must be clearly documented and appropriately coded to support medical necessity, even if the specialist is not actively managing that condition. If there is no bilateral designation but the problem exists on both the right and left sides, code both sides. For example, if the patient has secondary arthritis of both shoulders and laterality is not present in the code category, two codes are necessary.
M19.211 Secondary osteoarthritis, right shoulder
M19.212 Secondary osteoarthritis, left shoulder
Both would be reported.
Another situation seen far too often when performing audits is a lack of specificity and laterality in coding the encounter. Keep in mind that an unspecified diagnosis code can trigger an audit when more specific codes could have been used. For example, the physician codes unspecified foot pain (M79.673). A payor will most likely deny the claim because laterality is not coded. In actuality, when reviewing the documentation, the physician stated the patient has a non-displaced Fracture of the left 5th metatarsal shaft when the patient banged their foot against the coffee table at home. To support medical necessity and paint an accurate picture of the patient’s condition, this is how it should be coded:
S92.354A- Nondisplaced fracture of the fifth metatarsal bone, right foot, initial encounter for closed fracture
W22.03XA- Walked into furniture, initial encounter
Y92.009- Place of occurrence: home
Practitioners often code R52 (generalized pain) when more specific documentation exists. If the documentation states pain in the left wrist, it should be coded as M25.532 (pain in left wrist). When reporting pain diagnoses, the specific anatomic site and laterality must be identified.
It is also essential to link the diagnosis to the procedure code (CPT, HCPCS). The procedure and diagnosis must make sense together. For example, you can’t expect a payor to reimburse a provider when an echo was billed on the claim with a diagnosis of rhinitis. When bariatric surgery is performed on a patient with a diagnosis submitted on the claim as obesity, and the medical policy indicates the diagnosis supported is morbid obesity, the claim most likely would be denied. In both examples, it is clear that medical necessity is not supported.
Before submitting the claim, verify that each procedure is properly supported by the appropriate diagnosis code .Claims must be coded according to the patient’s actual medical condition(s), not based on payer coverage policies. Any selected diagnosis code should be based on the patient’s medical condition(s), even if the payor policy does not cover the service. If the service is not covered based on the diagnosis code, the patient should be informed that they will need to pay for the service. For Medicare, the ABN is an important document that must be signed for a procedure or service that might not be covered for that particular condition, and that allows the patient to decide whether to proceed with the service. If the ABN is not signed, the patient will not be responsible for payment of the service. Reporting a diagnosis that the patient does not have solely to obtain reimbursement for a service can result in an incorrect claim.
Ten Tips to Ensure Compliance with Medical Necessity
Review payer medical coverage policies for all procedures and services you perform at least annually. Many payers offer listservs or update alerts to which you can subscribe.
Ensure that documentation supports the specificity of each billed service and that all relevant diagnoses, including comorbidities affecting patient care are reported.
Link each procedure code to the appropriate diagnosis code that supports medical necessity. The relationship between the two must be clinically logical.
Make certain when the coding guidelines instruct “Use an additional code,” that you review the instructional notes in ICD-10-CM.
Query the practitioner when unspecified diagnoses are selected and obtain clarification.
Review medical payor coverage policies routinely to ensure that you are informed of diagnoses not covered under the policy.
When reporting an Evaluation and Management (E/M) service, ensure the level selected is supported by medical necessity.
Always review your denials to see if the denial is based on the diagnosis code. It could be that the denial is based on medical necessity or an invalid diagnosis code.
Make certain your diagnosis code contains the required characters and is coded to the highest level of specificity.
Perform periodic audits to validate that medical necessity is supported for each encounter. Educate the providers when problem areas are identified.
Every claim submitted to the payor must be coded accurately, medical necessity must be supported, and documentation must be clear, concise, and complete. The diagnosis codes reported in the progress note, operative report, or diagnostic study must accurately reflect the patient’s condition. Additionally, all comorbidities that impact patient care should be clearly documented and coded.
Sources:
Current Procedural Terminology (CPT, 2026); American Medical Association, CMS Pub. 100-4; chapter 12 section 30.6.1
Wikipedia
Empowering Your Practice with AI: Challenges and First Steps
Over the last 25 years, we have witnessed several industry evolutions from policy changes that altered the delivery of health care, advancement of medical therapies that have fundamentally changed patient outcomes, to the adoption of the Electronic Health Record (EHR). However, the AI evolution which we are experiencing may provide the most rapid and impactful progression to date. This evolution brings unprecedented leadership challenges and complex questions with no single answer.
Matthew Shortt, PA-C, MBA
Karen Zupko and Associates, Inc.
Over the last 25 years, we have witnessed several industry evolutions from policy changes that altered the delivery of health care, advancement of medical therapies that have fundamentally changed patient outcomes, to the adoption of the Electronic Health Record (EHR). However, the AI evolution which we are experiencing may provide the most rapid and impactful progression to date. This evolution brings unprecedented leadership challenges and complex questions with no single answer.
Many of the benefits of AI have been well documented, from intelligent patient management in which AI tools optimize patient scheduling and streamline patient flow minimizing patient wait time and improving patient outcomes. To one that is near and dear to me, AI tools and platforms aimed at preventing physician and provider burnout. While, yes, many of the challenges have been well documented as well, the path for healthcare leaders to embrace, implement, and optimize AI remains undefined. In thinking about this path, we have identified several of the challenges that exist and the first steps to get started in overcoming them as a modern healthcare practice leader.
The Challenges
Paradox of Choice. With the rapid proliferation of AI products entering the market, we have found this to be a gatekeeping step in many leaders’ AI journey. The number of products paired with the marketing hype in this space can create a sense of selection paralysis leading to delayed adoption and a fear of buyers’ remorse.
Integration, Interoperability, and Cost. With many practices still operating from their legacy EHR systems, that may seem like they were just adopted, integrating new AI tools and platforms can pose a significant and costly challenge to create compatible infrastructure.
Data Privacy and Security. We currently are operating in an environment of increasing cyberattacks and any one attack can cripple your medical practice. Ensuring new AI tools, which rely on immense amounts of patient data, operate under strict compliance regulations is imperative and anxiety inducing all in one.
Workforce Adoption. Once a new AI tool or platform has been selected, the new challenge of implementation and adoption arises. Recent reporting from KPMG indicates that up to 80% of healthcare AI initiatives fail citing poor change management and workforce cultural resistance.
First Steps
Start Talking About AI. While this may sound overly simplified, this is where it really starts. As a practice leader, you must be willing to have a conversation about AI and how you see it integrating into your practice. These conversations need to take place not only in the boardroom with your executive partners and physicians, but equally as importantly, in the break room with your entire team. These conversations should center on transparency, empathy, and collaboration while focusing on AI as a tool for growth and empowerment. A successful conversation will address any fears directly and welcome continued team member involvement and feedback.
Select an AI Champion(s). Depending on the size and complexity of your practice, this could be one individual or a committee of individuals, but regardless formally identifying and empowering an AI champion will serve as one, if not the most important steps in your AI success. This individual(s) will serve as your bridge builder, and their primary role should be to demystify AI driving adoption and engagement. If you are unable to identify an appropriate individual internally, there are numerous subject matter experts within our healthcare leadership ecosphere that provide these services. Your successful AI implementation will be a direct result of the time, training, and resources your champion(s) are allocated.
Define your AI Strategy. Just as you develop your practice budget, you should be developing and mapping your AI strategy for the next 1, 3, and 5 years. By surveying your clinical and administrative teams you will have a good understanding of where your biggest challenges and opportunities exist and pair these against potential AI tools to maximize your ROI. Once your goals have been identified your AI strategy will provide the roadmap to focus, align, and maintain your team’s effort as to navigate any challenge that arises on your AI journey.
Embrace Change Management. Your change management leadership will be crucial for navigating skepticism, fear, and the overall human element of AI adoption. Before any initiation of change, take the time to prepare your “people plan”, who is going to be involved and how are they going to be involved and how am I as their leader going to guide them through this evolution. Being prepared to provide reskilling and upskilling opportunities for your team members will not only garner more engagement but will provide you with more skilled team members to optimize your AI tools.
With healthcare changing and evolving faster than ever, the burden of current practice leadership is real and so is the opportunity. Those leaders and practices that embrace and champion AI into their practices and embrace change management initiatives will find themselves not only well positioned to thrive in our new healthcare landscape, but the ones writing the books about this next evolution.
Recognizing Burnout in Healthcare Staff and Ideas for Addressing It
Read the contributing factors to healthcare worker burnout and the results of a survey that assesses the factors of employment that healthcare workers most value. Using the results, we’ll present four best practices for reducing burnout and retaining employees.
By Synchrony, Health & Wellness
Read the contributing factors to healthcare worker burnout and the results of a survey that assesses the factors of employment that healthcare workers most value. Using the results, we’ll present four best practices for reducing burnout and retaining employees.
5 Ways to Help Improve Revenue Cycle Management
Revenue cycle management (RCM) is critical for health and wellness providers. Implementing RCM best practices could help you improve your patient experience and stay financially healthy.
By Maureen Bonatch M.S.N., R.N. and Suchi Rudra
Registered Nurse and Digital Writer
Revenue cycle management (RCM) is critical for health and wellness providers. Implementing RCM best practices could help you improve your patient experience and stay financially healthy. Read more.
The Rise of Automated Downcoding – White Paper
Physician practices are experiencing a sharp increase in systematic downcoding by major commercial payors. This trend, driven largely by AI-powered algorithms, is resulting in significant revenue loss, higher administrative burden, and frustration for practices.
The Rise of Automated Downcoding: Trends, Causes, and Strategies for Physician Practices
By Cathy McDowell, MBA, BSN
President and CEO
Karen Zupko & Associates, Inc.
August 2025
Executive Summary
Physician practices are experiencing a sharp increase in systematic downcoding by major commercial payors (1)(6). This trend, driven largely by AI-powered algorithms, is resulting in significant revenue loss, higher administrative burden, and frustration for practices.
Background
Beginning in late 2022, payors began using AI and machine learning to evaluate claims, replacing the largely manual, audit-driven downcoding process. By 2025, this technology had transformed downcoding into a routine, automated cost-control strategy, predicting justified service levels from structured claim data.
Current Trends (2025)
1. Targeted Services: Evaluation & Management (E/M) visits are the most common adjustments, along with telehealth services and split/shared visits (3)(4).
2. Payors Leading the Trend: UnitedHealthcare (3), Cigna (4), Aetna (5), Regional Blue Cross/Blue Shield, Humana (6).
Why Is This Happening?
Cost Containment (6), Post-2021 CPT Guideline Shifts (1), Peer Comparison Algorithms (4), Documentation Gaps (2).
Impact on Practices
Revenue erosion can result in six-figure annual losses for practices. The administrative burden of appealing each claim delays payment and increases costs, while physicians report growing frustration as AI-driven decisions occur without full record review (6).
Strategies for Practices
Recommended strategies include monitoring CPT submissions against paid codes by payer, validating documentation internally, appealing denials with strong evidence, and strengthening documentation templates and workflows (6)(1)(2).
Advocacy and Industry Response
The AMA and MGMA are advocating for transparency in AI-driven downcoding algorithms (1)(6). Specialty societies such as AAOS and ACS are preparing position statements. Regulatory agencies, including CMS, have required that Medicare Advantage plans provide justification for automated downcoding and ensure a fair appeals process (2).
The Path Forward
Practices must collect evidence of inappropriate systemic downcoding, appeal every automated downcode to create a documented pattern (6), and engage with professional societies to push for transparency and oversight.
Conclusion
Automated downcoding represents a significant shift in payer behavior. By tracking trends, enhancing documentation, consistently appealing, and participating in advocacy efforts, physician practices can mitigate financial damage while advocating for systemic reform (6)(2).
KZA stands ready to partner with practices to provide support through downcoding impact dashboards, audit documentation for appeals, internal documentation education, and templates with guidance for the appeal process.
References
1. American Medical Association. (2021). CPT® Evaluation and Management Guidelines.
2. Centers for Medicare & Medicaid Services. (2021). MLN Matters SE21002: Evaluation and Management Services.
3. UnitedHealthcare. (2024). Professional E/M Coding Policy.
4. Cigna. (2024). E/M Review Guidelines.
5. Aetna. (2024). Clinical Policy Bulletins.
6. Medical Group Management Association. (2025). Advocacy Updates on Downcoding and AI Algorithms.
Webinar: Tools for Financial Discussions with Orthopedic Patients
This webinar will dive into ways healthcare leaders can leverage digital solutions to create more opportunities for providers to engage with patients on topics that directly impact their experience such as financial discussions that may help increase patient satisfaction, loyalty and retention.
By Synchrony, Health & Wellness
This webinar will dive into ways healthcare leaders can leverage digital solutions to create more opportunities for providers to engage with patients on topics that directly impact their experience such as financial discussions that may help increase patient satisfaction, loyalty and retention.
Optimizing Orthopaedic Care: A Guide to Global-Period and Transfer-of-Care Modifiers
In the May 2025 AAOS Now practice management article, “Optimizing Orthopaedic Care: A Guide to Global-Period and Transfer-of-Care Modifiers,” Christine Banks, RHIA, CPC, CPCO, reviews the structure of the global surgical period and the importance of accurate documentation and coding to support continuity of care and proper reimbursement. The article explains how preoperative, intraoperative, and postoperative services are bundled within 0-, 10-, or 90-day global periods and how relative value units are distributed across each phase of care.
Christine Banks, RHIA, CPC, CPCO
Karen Zupko and Associates, Inc.
In the May 2025 AAOS Now practice management article, “Optimizing Orthopaedic Care: A Guide to Global-Period and Transfer-of-Care Modifiers,” Christine Banks, RHIA, CPC, CPCO, reviews the structure of the global surgical period and the importance of accurate documentation and coding to support continuity of care and proper reimbursement. The article explains how preoperative, intraoperative, and postoperative services are bundled within 0-, 10-, or 90-day global periods and how relative value units are distributed across each phase of care.
The article highlights expanded CMS documentation requirements in 2025 for cases in which postoperative care is transferred to another provider outside of the operating surgeon’s group practice. It provides detailed guidance on appropriate use of modifiers 54 (surgical care only), 55 (postoperative management only), and 56 (preoperative management only), as well as when evaluation and management services should be reported instead. The article also introduces HCPCS code G0559, which may be reported once per 90-day global period to capture postoperative follow-up work when no formal transfer of care has occurred.
This article offers practical insight for orthopaedic practices navigating global-period billing and transfer-of-care scenarios and reinforces the need for clear communication, proper documentation, and adherence to updated CMS guidelines to reduce compliance risk and support optimal patient outcomes.
Read the full article on AAOS Now:
Tools and Resources to Help Your Team Succeed
Get the support you need to simplify the financing conversation for your staff and your patients or clients. CareCredit offers in-office and online marketing materials, scripts, tools for calculating estimated payments and much more.
By Ilima Loomis
Digital Writer
Get the support you need to simplify the financing conversation for your staff and your patients or clients. CareCredit offers in-office and online marketing materials, scripts, tools for calculating estimated payments and much more.
ICD-10-CM Basics for Orthopaedics
In the July 2024 AAOS Now practice management article, “ICD-10-CM Basics for Orthopaedics,” Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC, outlines why diagnosis coding accuracy is critical to orthopaedic practices. The article explains how ICD-10-CM codes support medical necessity, reimbursement, patient complexity, and clinical research, and clarifies the distinction between CPT codes, which describe services performed, and ICD-10-CM codes, which explain why those services were provided.
Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC
Karen Zupko and Associates, Inc.
In the July 2024 AAOS Now practice management article, “ICD-10-CM Basics for Orthopaedics,” Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC, outlines why diagnosis coding accuracy is critical to orthopaedic practices. The article explains how ICD-10-CM codes support medical necessity, reimbursement, patient complexity, and clinical research, and clarifies the distinction between CPT codes, which describe services performed, and ICD-10-CM codes, which explain why those services were provided.
The article emphasizes the importance of clear, specific documentation, particularly as practices increasingly rely on EMRs and AI-assisted coding tools. Key areas of focus include laterality, acuity, injury status, comorbidities, social determinants of health, and proper use of seventh characters and Z codes. The article also highlights the ICD-10-CM chapters most relevant to orthopaedics and reinforces the need to follow official guidelines, indexes, and tabular lists when selecting diagnosis codes.
This article serves as a practical refresher for orthopaedic professionals and underscores the need for ongoing education, internal audits, and regular system updates to stay current with annual and interim ICD-10-CM changes.
Read the full article on AAOS Now:
Commonly Asked Orthopaedic Coding Questions in 2023
In the March 2024 AAOS Now article, “Commonly Asked Coding Questions in 2023,” Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC, addresses frequently encountered CPT coding questions from orthopaedic surgeons, practice managers, and coding professionals. The article provides practical clarification grounded in current CPT guidelines, NCCI edits, and payer-specific policies.
Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC
Karen Zupko and Associates, Inc.
In the March 2024 AAOS Now article, “Commonly Asked Coding Questions in 2023,” Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC, addresses frequently encountered CPT coding questions from orthopaedic surgeons, practice managers, and coding professionals. The article provides practical clarification grounded in current CPT guidelines, NCCI edits, and payer-specific policies.
Topics include appropriate reporting of spine procedures performed at the same level, correct use of modifier 59, coverage considerations for wound vac placement, dry needling, and biologic augmentation, as well as clarification on services that are not separately billable. Throughout, the article emphasizes accurate documentation and awareness of payer rules to reduce compliance risk.
This resource offers clear, real-world guidance for navigating common coding challenges in orthopaedic practices.
Read the full article on AAOS Now:
The Details of Denials Matter
It is interesting how orthopaedic surgeons react when they see a denial report for the first time. They often react first with surprise, followed by a perplexed question: “Why didn’t anyone inform me about this earlier?”
AAOSNow – Winter 2023
by Karen Zupko
It is interesting how orthopaedic surgeons react when they see a denial report for the first time. They often react first with surprise, followed by a perplexed question: “Why didn’t anyone inform me about this earlier?”
Concerning Error Rates Released on DME Billing
In the October 2023 AAOS Now article, “Concerning Error Rates Released on DME Billing,” Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC, highlights concerning Medicare error-rate data related to durable medical equipment (DME) billing in orthopaedic practices. Reported error rates were notably high for commonly dispensed items, including ankle-foot orthoses, knee orthoses, and spinal orthoses, underscoring significant compliance and revenue risks.
Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC
Karen Zupko and Associates, Inc.
In the October 2023 AAOS Now article, “Concerning Error Rates Released on DME Billing,” Marissa Clemmer, CPC, CCS, CPMA, CPB, CANPC, CPEDC, highlights concerning Medicare error-rate data related to durable medical equipment (DME) billing in orthopaedic practices. Reported error rates were notably high for commonly dispensed items, including ankle-foot orthoses, knee orthoses, and spinal orthoses, underscoring significant compliance and revenue risks.
The article outlines common reasons for DME claim denials, such as incorrect HCPCS codes, missing or incomplete documentation, lack of medical necessity support, and failure to meet local coverage determination (LCD) requirements. It emphasizes that these errors can result in delayed or lost reimbursement for already-dispensed equipment, creating substantial financial impact for practices.
To reduce risk, the article recommends steps orthopaedic practices can take to improve DME billing compliance, including understanding DME MAC requirements, maintaining thorough documentation, staying current on payer guidelines, responding promptly to audit requests, and training staff on proper use of written orders and proof of delivery. This article serves as an important reminder of the need for strong DME processes to protect both compliance and revenue.
Read the full article on AAOS Now:
The Details of Denials Matter
In the September 2023 AAOS Now practice management article, “The Details of Denials Matter,” Karen Zupko examines the often-overlooked impact of claim denials on orthopaedic practices and emphasizes the importance of routinely reviewing and sharing denial data with surgeons and staff. The article explains how a lack of transparency around denials breaks the feedback loop and prevents meaningful improvement in billing and documentation practices.
Karen Zupko
Karen Zupko and Associates, Inc.
In the September 2023 AAOS Now practice management article, “The Details of Denials Matter,” Karen Zupko examines the often-overlooked impact of claim denials on orthopaedic practices and emphasizes the importance of routinely reviewing and sharing denial data with surgeons and staff. The article explains how a lack of transparency around denials breaks the feedback loop and prevents meaningful improvement in billing and documentation practices.
The article highlights common contributors to denials, including incomplete documentation, late filing, registration errors, unbundling issues, and understaffing, noting that denials frequently occur even when coding appears technically correct. By analyzing denial reason codes, practices can identify patterns, pinpoint training gaps, and uncover significant revenue leaks that may otherwise go unnoticed.
This article reinforces that denial management is a shared responsibility between surgeons and staff and demonstrates how regular review of denial reports can lead to fewer appeals, reduced write-offs, and measurable financial improvement for orthopaedic practices.
Read the full article on AAOS Now:
What Orthopaedic Surgeons Should Know about Medicare Audits in 2023
In the September 2023 AAOS Now practice management article, “What Orthopaedic Surgeons Should Know about Medicare Audits in 2023,” Matthew Twetten, MA, MHCDS, outlines key updates and considerations related to Medicare claims audits. The article explains why audit activity remains a significant compliance risk for orthopaedic practices and highlights how Medicare’s program integrity efforts are designed to identify improper payments, fraud, waste, and abuse.
Matthew Twetten, MA, MHCDS
Karen Zupko and Associates, Inc.
In the September 2023 AAOS Now practice management article, “What Orthopaedic Surgeons Should Know about Medicare Audits in 2023,” Matthew Twetten, MA, MHCDS, outlines key updates and considerations related to Medicare claims audits. The article explains why audit activity remains a significant compliance risk for orthopaedic practices and highlights how Medicare’s program integrity efforts are designed to identify improper payments, fraud, waste, and abuse.
The article reviews the various types of Medicare audit contractors, including Medicare Administrative Contractors (MACs), Recovery Audit Contractors (RACs), CERT contractors, ZPICs, PSCs, and Supplemental Medical Review Contractors (SMRCs), and explains how each conducts reviews and requests documentation. It also clarifies how audit targets are established, including the role of CMS and the HHS Office of Inspector General, and identifies areas of heightened scrutiny such as trauma claims, evaluation and management services, and telehealth.
This article provides valuable context for orthopaedic practices seeking to understand the Medicare audit landscape and reinforces the importance of proactive compliance, accurate documentation, and regular internal review to reduce audit risk.
Read the full article on AAOS Now:
Simple Patient Financing Solutions for Maximizing Treatments
Many aesthetic practices and spas we work with offer patient financing—but you’d never know it. Either there’s nothing mentioned on the Web site or it’s like an Easter egg hunt to find the information. When scheduling, patients raising concerns or questions about fees—are rarely told that financing is offered. Many practices wait and discuss financing only after a patient is seen and wants to schedule. It’s big mistake.
Aesthetic Society News – Fall 2022
by Karen Zupko
Many aesthetic practices and spas we work with offer patient financing—but you’d never know it. Either there’s nothing mentioned on the Web site or it’s like an Easter egg hunt to find the information. When scheduling, patients raising concerns or questions about fees—are rarely told that financing is offered. Many practices wait and discuss financing only after a patient is seen and wants to schedule. It’s big mistake.
CMS Updates Physician Assistant and Nurse Practitioner Billing
In January, CMS introduced guideline changes to its Medicare reporting rules that impact PA/NP billing. These changes could require practices to modify how they report split/shared services. Previously, shared services were frequently reported in the name of a physician. Now, new rules determine who can report the services. Failing to comply with the new CMS rules will create compliance risks for physician practices.
AAOSNow – May 2022
by Sarah Wiskerchen
In January, CMS introduced guideline changes to its Medicare reporting rules that impact PA/NP billing. These changes could require practices to modify how they report split/shared services. Previously, shared services were frequently reported in the name of a physician. Now, new rules determine who can report the services. Failing to comply with the new CMS rules will create compliance risks for physician practices.
Disclaimer: Full article requires AAOSNow login.
Commonly Asked Coding Questions in 2022
In this column, KZA addresses recently asked questions on coding for various orthopaedic procedures posed by orthopaedic surgeons, practice managers, and staff.
AAOSNow – March 2022
by Sarah Wiskerchen
In this column, KarenZupko & Associates addresses recently asked questions on coding for various orthopaedic procedures posed by orthopaedic surgeons, practice managers, and staff.
Disclaimer: Full article requires AAOSNow login.
Op Note Documentation Tips Every Surgeon Can Use
You’ve submitted, in a timely manner, correct Current Procedural Terminology® (CPT) codes to the insurance company for the procedure you performed. The payor’s explanation of benefits (EOB) or electronic remittance advice (ERA) shows a payment of $0! Now what? Typically, you’d send in the operative note, showing the description of the procedure you performed.
You’ve submitted, in a timely manner, correct Current Procedural Terminology® (CPT) codes to the insurance company for the procedure you performed. The payor’s explanation of benefits (EOB) or electronic remittance advice (ERA) shows a payment of $0! Now what? Typically, you’d send in the operative note, showing the description of the procedure you performed.
The operative note is not only a medico-legal and patient care document. It’s usually the only information a payor wants when there is a dispute about your reimbursement.
So let’s walk through some key elements of the operative report documentation.
Pre-operative and Post-operative Diagnoses
All relevant pre- and post-operative diagnoses should be documented, including underlying co-morbid conditions that you consider relevant for the procedure performed. If a pre-op diagnosis is no longer relevant, or changes intra-operatively, then state this in the post-operative diagnosis statement.
For example, if the tumor or lesion pathology is not known pre-operatively, it is acceptable to state “unknown” in the pre-op diagnosis. If the frozen section comes back positive for a malignancy, this could be stated in the post-op diagnosis area.
Surgeon
The primary surgeon for the procedure is listed as the surgeon. In the academic environment, this is the attending surgeon for the procedure.
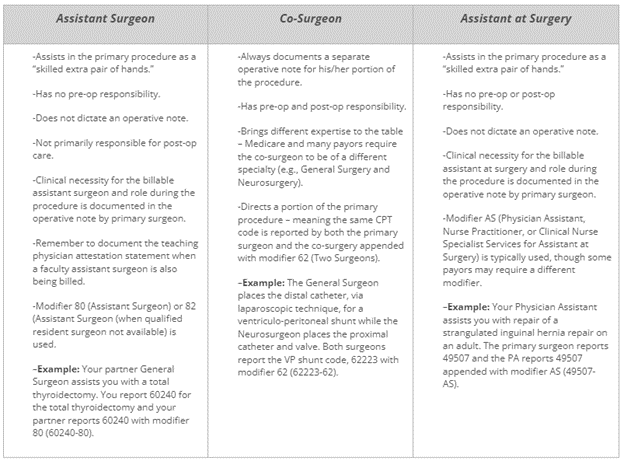
Assistant Surgeon vs. Co-Surgeon vs. Assistant at Surgery
Not crystal clear on the difference? Here are some tips that describe the different surgical roles typically seen in a procedure.
Procedure(s) Performed
The procedures performed are listed in this area of the operative note, which is typically on the top half of the first page. We recommend using CPT terminology as much as possible, but not including codes in the operative note. Why? Oftentimes, the codes documented in the operative note are not accurate.
It becomes a compliance issue when the codes in the operative report do not match the codes billed on the CMS 1500 claim form. Medicare’s General Principles of Medical Record Documentation state the CPT and ICD-10-CM codes reported on the health insurance claim form or billing statement should be supported by the documentation in the medical record. When a CPT code is documented in the operative report but not billed the CPT code billed is not “supported by the documentation in the medical record” as Medicare requires.
Indications for Surgery
This short paragraph, a couple of sentences, is very important as it provides the clinical necessity for the procedure being performed. It is also important to state any previous, related surgery on the same or different structure/wound, why patient is being brought back to the OR, or planned future surgery, as these are clues that coders use to support specific modifiers.
For example, a patient may require stages, of surgery to reconstruct an open wound which would warrant use of modifier 58 (Staged or Related Procedure or Service by the Same Physician or Other Qualified Health Care Professional During the Postoperative Period). Stating clearly that the staged procedures are prospectively planned, in this case, would tell the coder and payor that modifier 58 is warranted and the full allowable should be paid. All too often, when the planned nature of multiple procedures is not documented, a modifier 78 (Unplanned Return to the Operating/Procedure Room by the Same Physician or Other Qualified Health Care Professional Following Initial Procedure for a Related Procedure During the Postoperative Period) is used, which generally results in a payment reduction.
Complexity
This separate paragraph is a must if modifier 22 (Increased Procedural Services) will be used to obtain additional payment. This information should summarize the added complexity that will be in the subsequent details documented in the operative note. Don’t expect a payor to wade through the details of the operative note to try to figure out whether to pay you more. Make it easy for the payor to “feel your pain” of the procedure in a Complexity, or Findings at Surgery, paragraph.
Details or Description of Procedure
This is typically the lengthiest area of the operative note that describes the procedure(s) performed in great detail. Documentation should include, but not be limited to, induction of anesthesia, patient positioning, set-up and use of special equipment (e.g., stereotactic navigation, robot), specific brand name of any implant(s), which surgeon did what when more than one surgeon is involved, etc.
The details in this section of the operative note should support the procedures listed in the aforementioned Procedure(s) Performed area, which should also support the CPT code(s) reported for the procedure(s).
6 Essential Coding Rules Everyone Needs to Know
Current Procedural Terminology® (CPT) is a coding system that physicians and other providers use to bill for their services. While typically not taught in medical school, residency or other formal education arenas, providers are still expected to know how to properly code for services provided.
Current Procedural Terminology® (CPT) is a coding system that physicians and other providers use to bill for their services. While typically not taught in medical school, residency or other formal education arenas, providers are still expected to know how to properly code for services provided.
Here are six basic coding rules that apply to all specialties and that every provider, manager, billing, and coding staff must follow. Understanding the basics will help providers code accurately and reduce the risk of an audit or insurance company takeback or refund.
1. Do not report multiple CPT codes when a single comprehensive code describes these procedures. Doing so is called “unbundling.”
For example, there are codes that describe a tonsillectomy and adenoidectomy performed at the same operative session (42820-42821). It is considered “unbundling” if two separate codes are reported – one for the tonsillectomy (42825-42826) and one for the adenoidectomy (42830-42836).
Another example is use of the exploratory laparotomy code, 49000. An exploratory laparotomy is included in all other laparotomy codes; therefore, 49000 would not be separately reported. To do so is considered “unbundling” because the more comprehensive code includes the exploratory laparotomy.
2. Avoid “upcoding.” Do not report a “higher” code when a “lower” code is more accurate.
“Upcoding” oftentimes occurs when reporting Evaluation and Management (E/M) codes for office and hospital non-surgical services. If the documentation supports 99203 (new patient visit, level 3), it is considered “upcoding” if the provider codes the service as a higher level such as 99204 (new patient visit, level 4).
3. Remember that there are services integral to a CPT code. Refer to CPT guidelines and your physician specialty publications for more information.
CPT guidelines are not very specific about the services integral to a surgical procedure code. From an intraoperative standpoint, CPT states only the “local infiltration, metacarpal/metatarsal/digital block or topical anesthesia” is included. The assumption is that services normally performed as part of a single CPT code would not be separately coded.
The lack of specificity in CPT has led several physician specialty societies to publish their own guidelines for members and coders.
A good example is performing a lumbar discectomy with use of fluoroscopy for disc space localization. The American Academy of Orthopaedic Surgeons’ Code-X, as well as the American Association of Neurological Surgeons Guide to Coding, state that fluoroscopy is included in all open surgical procedure codes and not separately reported as shown in the table below.
| Correct | Incorrect |
|---|---|
63030 Lumbar discectomy |
63030 Lumbar discectomy |
76000 Fluoroscopy |
4. Access or exposure (e.g., approach), is included in all surgical CPT codes with one exception.
CPT codes describe complete procedures. The incision/exposure/approach to the level of the pathology is included in all surgical procedure codes and should not be separately coded. The American Academy of Orthopaedic Surgeons’ Code-X and the American Association of Neurological Surgeon’s Guide to Coding are examples of how physician specialty societies have specifically defined that the access or approach to the procedure is included in the CPT code.
For example, the endoscopic intranasal approach to a pituitary tumor is included in 62165 (endoscopic transnasal excision of a pituitary tumor). When the otolaryngologist performs the endoscopic intranasal approach for the neurosurgeon to excise the pituitary tumor, then each surgeon reports the same CPT code with modifier 62 (Two Surgeons). The exposure/approach is included in 62165, a stand-alone CPT code, and should not be separately reported with component codes as shown in the table below.
| Correct | Incorrect |
|---|---|
62165-62 |
Neurosurgery: |
Endoscopic pituitary tumor removal (co-surgery modifier) |
62165 Endoscopic pituitary tumor removal billed by neurosurgery |
ENT: |
|
30520 Septoplasty |
|
31287 Sphenoidotomy |
Another example is in spine surgery. The approach, or access, to the spine is included in all open spine surgical CPT codes. For example, the retroperitoneal approach is included in 22558 (anterior lumbar interbody fusion) because the procedure could not be accomplished without it. Therefore, when the vascular or general surgeon performs the approach – which is included in 22558 – the code is appended with modifier 62 and reported by both the approach and spine surgeons. It is not accurate for the approach surgeon to report a code such as an exploratory laparotomy (49000).
One exception: the skull base surgery codes (61580-61616) are separated into approach (61580-61598) and definitive procedure (61600-61616) for the resection and closure.
5. The usual closure is included in all surgical procedure CPT codes.
What is the “usual” closure? Well, that depends on the surgical procedure code. All surgical codes include the direct, or primary, closure where the wound edges of the operative tract created by the surgeon are closed primarily at the same operative session.
In general, my simple rule applies: if you open it, you’re supposed to close it.
Some codes may have language that closure is not included. In those instances, closure is typically not performed because the operative wound size is small such as in 41110 (excision of lesion of tongue without closure).
The excision of benign (114xx) and malignant (116xx) skin lesion codes includes a simple, or single layer, closure. If the closure qualifies for an intermediate (12031-12057) or complex (13100-13153) closure, it may be separately reported with the skin lesion excision code.
6. A “scout” endoscopy, diagnostic service, or exploratory procedure is included in a definitive CPT code performed at the same operative session.
Another of my simple rules is, if you are coding for cutting it out, you would not code for diagnosing or finding it.
For example, if you are doing a laryngectomy (31360), then the scout laryngoscopy to assess extent of disease and landmarks (31525) performed at the same operative session is included in the laryngectomy code and not separately reported.